INTRODUCTION
Inflammatory bowel diseases (IBD), mainly including UC and CD, are characterized by chronic progressive inflammation of the bowel.1 Although IBD was once considered a rare disorder in Asia compared with Western countries, the incidence and prevalence of IBD in Asia have been recently increasing. The population-based Korean data showed that the mean annual incidence rates of CD and UC increased from 0.05 and 0.34 per 100,000 persons, respectively, in 1986-1990 to 1.34 and 3.08 per 100,000, respectively, in 2001-2005.2
Growing evidence shows that the characteristics of IBD patients differ in epidemiology, phenotype, and genetic susceptibility according to geography.3 This variability of IBD across different countries may induce the variation in the practice pattern of different health-care systems, resulting in considerable divergence in patient outcomes. Therefore, it is timely to pay more attention to the quality improvement of IBD care. However, first, it would be a prerequisite to assess the levels of variation in IBD care among different countries. For this purpose, the IBD study group of the Korean Association for the Study of Intestinal Diseases (KASID) conducted a brief multinational survey for physicians who treat IBD patients in Asian countries, to identify disparities in their daily practice pattern on the occasion of the second annual meeting of the Asian Organization for Crohn's and Colitis (AOCC).
As there is no single gold standard for the diagnosis of IBD, it is a great challenge for clinicians to correctly diagnose these diseases. In the Asian geographic area, it is even more difficult to make accurate diagnosis of IBD because of various infectious diseases that mimic IBD, which may delay the accurate assessment of the clinical characteristics of the disease, leading to failure of early detection and appropriate management. For instance, intestinal tuberculosis (TB), which is relatively prevalent in Asian countries, is very similar to CD in terms of clinical symptoms, disease location, endoscopic appearance of mucosal ulcerations, and pathologic feature. Thus, this study was focused on identifying how Asian physicians approach patients with suspected IBD for the correct diagnosis through a multinational survey in the region.
METHODS
This survey was originally planned by the organizing committee of the AOCC and designed for one of the programs of the second annual meeting of AOCC, which was held in Seoul in June 2014. The questionnaire used in this study was made by members of the IBD study group of KASID. Then, it was revised several times after being reviewed by the staff officer members of KASID and their colleagues from Japan and China. It mainly consisted of four parts, including personal information (9 items), diagnosis of IBD (18 items), treatment of IBD (30 items), and quality of IBD care (36 items). For the diagnosis of IBD, questions were asked about the most commonly used diagnostic guidelines and disease activity assessment systems, whether or not to apply the Montreal classification, and the available tools for small-bowel or perianal disease evaluation for CD. The questionnaires are shown in the Appendix. The survey was conducted through a web-based system between March 2014 and May 2014. The questionnaire was sent to medical doctors caring for IBD patients in Asia via e-mail by representative members for each Asian country in the organizing committee of the AOCC. The results of treatment and quality of IBD care will be reported elsewhere.
RESULTS
1. General Information of Participants
Overall, 353 Asian medical doctors (male, 251 [71.1%]) who treat IBD patients responded to the survey. Most of them were working in academic teaching hospitals (336 [95.2%]). The respondents were from various Asian countries (Korea 116, China 114, Japan 88, Taiwan 17, Hong Kong 8, India 4, Singapore 3, Malaysia 1, the Philippines 1, and Indonesia 1).
2. Diagnostic Guidelines and the Montreal Classification
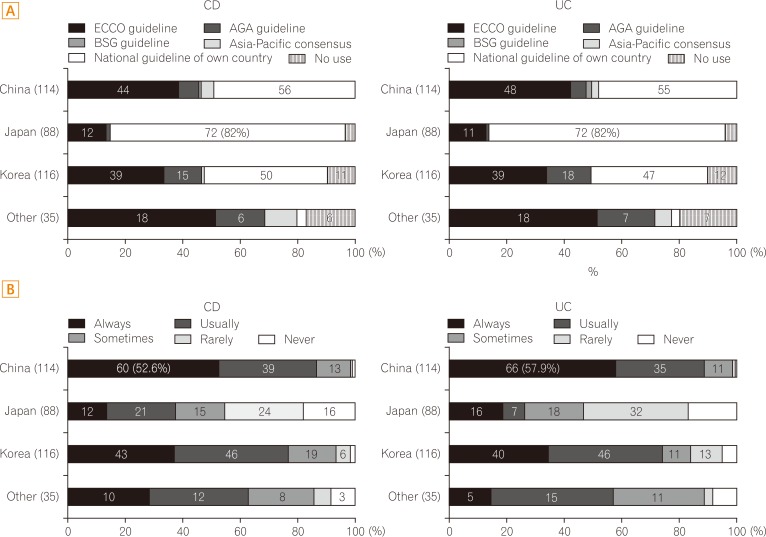
The national diagnostic guideline for IBD is the most commonly used guideline among respondents from Korea, China, and Japan. Physicians from the other countries apply the European Crohn's Colitis Organisation's guideline most frequently (Fig. 1A). The least number of Japanese physicians classify their IBD patients according to the Montreal classification compared with those from Korea, China, and other Asian countries (Fig. 1B).
3. Clinical, Endoscopic, and Radiologic Assessment Tools
For the index or scoring system for the clinical assessment of disease activity of UC, all respondents favor the Mayo score except those from China. The Truelove-Witts index is the most commonly used system for UC activity assessment by Chinese doctors (Fig. 2A). For CD, the CDAI was overwhelmingly chosen by participants from all countries.
Although most physicians (72%-88%) from all countries always use endoscopic examination for evaluating disease activity and extent at the time of diagnosis of UC (Fig. 2B), only 22.8% to 68% of doctors answered that they always adopt an endoscopic severity classification system such as the Mayo endoscopic subscore or UC endoscopic index of severity (UCEIS) (Fig. 2C).
More than 90% of respondents from all countries perform colonoscopy with terminal ileum evaluation to document the activity and extent of disease for suspected CD (Fig. 2B). For small-bowel evaluation, however, there was a wide range of variation among countries. Physicians from Korea and China predominantly perform CT enterography, whereas those from Japan prefer small-bowel follow-through or balloon-assisted enteroscopy. Small-bowel follow-through is also the most frequently favored tool by doctors from the other countries, followed by CT enterography (Fig. 2D). Concerning perianal evaluation, pelvic MRI is the most commonly used instrument in all countries.
4. Evaluations for Excluding Infectious Diseases
For suspected UC, more than half of doctors from China and Japan reported to always perform microbiological culture, whereas only 11.2% and 25.7% of doctors from Korea and the other countries do, respectively (Fig. 3A). Clostridium difficile toxin assay is not conducted adequately in all countries; only 18.9% to 36% of respondents always perform stool C. difficile toxin assay for suspected UC (Fig. 3B).
Many physicians in Asia administer empirical anti-TB medications before the diagnosis of CD. Approximately 44.7%, 8%, 19.8%, and 17.1% of respondents from China, Japan, Korea, and the other countries, respectively, reported that >20% of their patients with CD had been administered with anti-TB treatments before the diagnosis of CD (Fig. 3C).
DISCUSSION
The results of this survey demonstrate a diverse approach for the diagnosis of IBD among Asian physicians, especially in terms of the kind of guidelines, adoption of the Montreal classification, and modality of small-bowel and perianal evaluation of CD. This study, on the occasion of the second AOCC in 2014, was conducted with 353 physicians, the largest number of participants to date for the survey investigating the pattern of practice of IBD care.
It has been recognized that there are various differences in phenotypes, epidemiologic features, and genetic backgrounds among CD patients from different countries, especially between the Western and Eastern geographic areas.4 Therefore, although well-established guidelines were developed early in Western countries on the basis of numerous evidences, they might not be fit for Asian IBD patients. In an effort to address this issue, individual diagnostic guidelines, criteria, and consensus on IBD have been developed in Asian countries, including China, Korea, and Japan in recent years.5,6,7,8 The result of the present study—that doctors from China, Korea, and Japan most commonly use their own national guidelines—mirrors the effort of the regional medical society to make significant improvement in the correct diagnosis of IBD in the Asian geographic area. For instance, Asian guidelines have included intestinal Behcet's disease and intestinal TB, as critical differential diseases that are relatively prevalent in these countries compared with their Western counterparts.5,6,8
Interestingly, the results of the present survey show that the Montreal classification of IBD is less used by doctors from Japan than those from other Asian countries. In fact, the Vienna or Montreal classification is not stated in the Japanese guidelines,6 whereas the Korean and Chinese guidelines or consensus take this classification into account.2,8 However, the exact reason for this lower use of the Montreal classification of IBD by Japanese doctors is unclear.
For the system of UC activity index, the Mayo score is dominantly used by most doctors except those from China, who answered to mainly adopt the Truelove-Witts score. The simplicity of the Truelove-Witts score might be one of the explanations for the preference of Chinese doctors to this scoring system, as this system does not need endoscopy for the calculation of activity.9 Meanwhile, the Mayo score requires the endoscopic evaluation of the mucosa for the calculation of activity.10 For CD, the CDAI is overwhelmingly favored by doctors from all countries. Considering the complexity and impracticability of CDAI,11 however, it remains to be seen how often physicians actually use CDAI in real clinical practice.
No endoscopic score system for UC has been widely used in daily routine practice. Although the Mayo endoscopic subscore has been extensively used in many trials,10 it has not been properly validated.12 Only the UCEIS and the UC colonoscopic index of severity (UCCIS) were recently validated.13,14 However, these new instruments are still not ready for use and not reliable as the definition of remission is lacking.14,15 This issue is well reflected by the result that respondents seldom use an endoscopic scoring system such as the Mayo score or UCEIS, whereas they answered to always perform an endoscopic examination for UC diagnosis, indicating the impracticability of the endoscopic scoring system. It is urgent to develop a novel clinical endoscopic score system that is well validated and simple to use.
It is notable that evaluation for C. difficile infection is not performed adequately by doctors from Asian countries; approximately only 30% of respondents perform C. difficile toxin assay for suspected UC (Fig. 3B). Recent Western epidemiologic studies have demonstrated that patients with IBD are greatly susceptible to C. difficile infection compared with the general population, prompting to recommend routine stool screening for C. difficile toxin in IBD patients.16,17 However, this trend seems to be not evident in Asian IBD patients, as there have been no data on this relation. It is not clear whether this lack of relation between C. difficile infection and IBD in Asia might be attributed to the lower prevalence of IBD compared with Western countries.
We found a significant range of variation in the evaluation of the small bowel for CD among countries. Korean and Chinese physicians favored CT enterography, whereas Japanese and those from other countries chose small-bowel follow-through as the first-line tool for assessing small-bowel lesions in CD patients. Notably, a considerable proportion of Japanese doctors (28.4%) use balloon-assisted enteroscopy, whereas no physicians in Korea prefer this modality (Fig. 2D). This difference might result from the various medical insurance systems or the level of accessibility to radiologic equipment in each country. For instance, balloon-assisted enterography is not reimbursed by the Korean national medical insurance, leading to a low preference for this tool among physicians.
One of the distinguished findings of the present study is the high rate of empirical anti-TB treatment before CD diagnosis in Asia, reflecting the difficulties in discriminating these two diseases. Although there have been several studies on the typical features of intestinal TB for differentiating it from CD,18,19,20,21,22,23 correct diagnosis is still challenging for physicians in the Asian geographic area. This result indicates the urgent need for a coordinated and organized effort to develop effective tools or markers to distinguish these two diseases in the region.
In conclusion, the results of the present survey demonstrate that Asian doctors apply different approaches to their IBD patients, reflecting a unique situation in this region compared with Western countries. It would be important to establish Asian guidelines for improved care of IBD patients.