INTRODUCTION
The age of presentation of IBD is increasingly more common under the age of 16 years [1,2]. IBD presenting at a young age is also more extensive and severe than in adults [3]. Hence, it is of utmost importance to ensure proper transition of care to the adult gastroenterologist.
In the context of healthcare, transition is defined as the purposeful, planned movement of adolescents with chronic physical and medical conditions to adult-orientated healthcare systems [4].
Transition of care for patients with IBD is commonly viewed as a period fraught with challenges for the patients, caregivers and healthcare providers alike. Many studies have shown the efficacy of a standardized transition program [5,6], and hence major organizations such as the European CrohnŌĆÖs and Colitis Organisation (ECCO) [7] do recommend a transition program for every adolescent. Moreover, ECCO states that IBD patients taking part in a transition program are likely to have better compliance and less adverse outcomes after transfer to adult care compared with those who do not take part. However, there is a lack of clear guidelines on the specific recommendations for a standardized transition program.
The authors believe that this may be attributed to the differences in the needs and expectations of IBD patients worldwide. Adolescence is a precarious period for growth and change, and the adolescent must shed the sheltered environment of childhood and achieve self-reliance and self-dependent living. Coupled with cultural differences and extent of parental involvement in patientsŌĆÖ care, it is evident that various societies require different levels of intensity for a transition program. Pediatric and adult gastroenterology clinics also have different areas of focus that changes with each stage of the patientŌĆÖs life. For example, pediatric clinics may be better able to deal with adolescent issues such as growth and puberty, exam pressure, sexual or recreational drug experimentation, whereas adult gastroenterologists are better geared towards tackling adult issues of fertility, family planning and surveillance of secondary conditions (e.g., malignancy and osteoporosis). Hence, it is fundamental that patients receive the appropriate care at each stage.
This paper is a review of the various studies that have been performed thus far, and aim to look into the basic requirements of a successful transition program. We also aim to identify the barriers to seamless transfer, with special mention of characteristics that are particular to the Asian population.
METHODS
A literature search on PubMed and Google Scholar was conducted with the keywords ŌĆ£IBD,ŌĆØ ŌĆ£transition,ŌĆØ ŌĆ£pediatric,ŌĆØ ŌĆ£transitional careŌĆØ and ŌĆ£transition clinic.ŌĆØ This search brought up a total of 37 relevant articles. The authors then went through the articles and summarized the pertinent points in this review.
PERCEPTION OF DOCTORS, CAREGIVERS AND PATIENTS ON TRANSITION
Many of the studies reviewed had polls on medical providers about their perception of transition care. It is not surprising that majority viewed a structured transition program to be very important [5]. However, a majority of medical providers also did not have a defined protocol for transition [5]. We find that having a structured transition program is beneficial to the stakeholders involved in the various ways as elaborated on in the points mentioned below.
Adolescents also require more attention during the transition period. A retrospective case-control study [3] compared disease characteristics and compliance in 100 adolescents with adult controls matched for disease duration. All adolescents were seen at a biweekly transition clinic of IBD patients ages 16-24 years old. A greater percentage of adolescents required hospital admission (46% compared to 14% of adults, P< 0.0001), azathioprine (46% compared with 17% of adults, P< 0.0001), and infliximab (20% compared with 6% of adults, P< 0.05). Adolescents missed a median number of 20% of their appointments compared with 0% in adults (P< 0.0001). This study shows that adolescents have more severe disease that may be due to primary noncompliance or the disease characteristics itself.
REQUIREMENTS OF A SUCCESSFUL TRANSITION PROGRAM
The following is an outline of the structured program that we propose for transition.
1. Multidisciplinary Team Meetings
Transition to self-management involves gradual changes in knowledge, attitudes, and behavior. This requires a multidisciplinary team (including pediatric and adult gastroenterologists, surgeons, parents/caregivers, school workers, nurses, dieticians, counselors, social workers, psychologists, healthcare systems, pharmacists, etc.) whose roles are all essential for seamless continuation of an adolescentŌĆÖs healthcare. Recognition of the roles of these individuals in multidisciplinary care and maximization of communication among them is of strategic importance.
These meetings should be scheduled on a regular basis, and not only in the short months leading up to the planned transfer of care for identified patients. At our center, team meetings between the pediatric and adult IBD teams are scheduled regularly on a 1 to 2 monthly basis. These meetings not only provide a proper place and avenue for discussion of transition cases, but also serve as a time for education and discussion of challenging pediatric and adult IBD cases. Furthermore, since the adult gastroenterologist will eventually take over the care of the patient, it makes sense for him/her to get involved early on in the management of these pediatric patients.
2. Alternating Visits between the Pediatric and Adult Clinic before Official Transfer
The aim of these alternating visits is to encourage patient autonomy and individual decision making while still providing some amount of handholding in the familiar background of the pediatric clinic. However, the final visit should be held in the adult gastroenterology clinic, but with the pediatric IBD nurse present.
We would like to emphasize on the importance of having a specialized IBD nurse in this transition process. The IBD nurse is the familiar face for patients and caregivers, and they also provide an invaluable resource for patients to contact should they have additional questions that were not addressed in the clinic. At our center, our IBD nurse is in charge of the IBD hot-line-an easy mode of contact for patients, especially if they are experiencing high burden of symptoms or are dealing with adverse effects of therapy. It has also potentially avoided unnecessary inpatient admissions and unscheduled clinic visits.
An Israeli group consisting of an IBD tertiary referral center in Tel Aviv conducted a study [6] on 36 patients (mean age, 19 ┬▒ 1.8 years) found that standardized transition clinics helped to improve self-efficacy scores in the ŌĆ£IBD-yourselfŌĆØ questionnaire. Their transition protocol included an average of 3 to 4 meetings over 6.9 ┬▒ 3.5 months. Self-efficacy scores in all domains of the questionnaire were significantly higher after completion of the transition.
During these visits, we propose that the IBD team, together with the patient and his/her caregiver, come up with a written healthcare transition plan that is updated with each clinic consult. Leung et al. [8] proposed a checklist of knowledge and tasks that adolescents should master before they transition fully to an adult care clinic. These include: (1) diagnosis (CD, UC, indeterminate colitis); (2) anatomic location of their disease; (3) extraintestinal manifestations; (4) year of diagnosis, and names of their IBD institutions/hospital/healthcare providers; (5) dates of hospitalizations, why they were hospitalized, events during hospitalizations; (6) dates of surgery and the procedure performed; (7) complications of their disease or therapy, e.g., fistulas, abscesses, opportunistic infections, pancreatitis, cytopenias; (8) names and doses of drugs they are currently on and have taken in the past; (9) insurance plan and contact information; (10) can make arrangements for blood tests and understands who to call for follow-up on the results; (11) calls the appropriate healthcare provider in the event of a disease flare; (12) calls the appropriate healthcare provider to refill medications; (13) can schedule their own visits and remembers to attend; (14) understands which medications can potentially be harmful during pregnancy and the need to discuss with healthcare provider issues regarding contraception and planning for children.
3. Proper Documentation of Medical Records
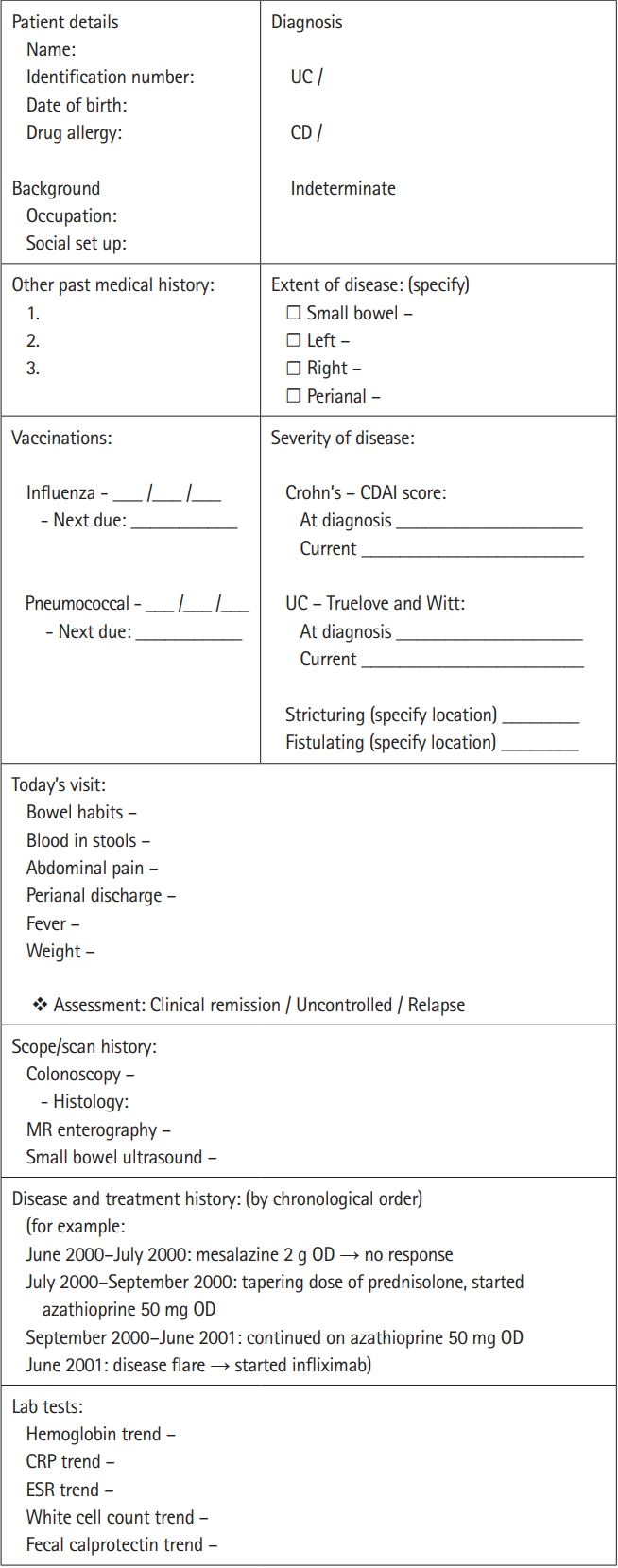
This point is often overlooked by physicians, but it is truly a fundamental component. Organized record keeping allows for easy access and retrieval of medical information, which is crucial for chronic diseases. The management of IBD, in particular, involves multiple lines of treatment-something which the patientŌĆÖs physician needs to be well-aware of what the patient has previously tried or failed before-so that the next line of treatment may be offered. The meticulous tracking of previous endoscopy findings, vaccination records, and lab/stool tests is also important since the follow-up of IBD patients usually go on for many years. We propose the implementation of standardized template for documentation (Fig. 1).
4. Determining the Ideal Timing for Transition
The ECCO review suggests that transition is best initiated in early adolescence [7]. In European countries, the transfer of care is at the age of 18 years, but in the United States, this is often at the age of 21 years or even up to 25 years [9]. In the Asian context, adulthood may be considered at age 21 years and above.
At the point of transfer of care, it is ideal if the patient were in clinical remission, or at the very least, have only clinically mild disease. During each clinic visit, a medical summary and an emergency plan should be reiterated, especially for patients who are symptomatic of active disease.
We also emphasize the importance of setting goals and deadlines for transfer of care.
DIFFERENCES BETWEEN THE NEEDS OF THE WESTERN AND ASIAN ADOLESCENT IBD POPULATION
The key difference lies in the different ages that major life events occur for Asian and Western populations. These ŌĆ£major life eventsŌĆØ include graduation, entering further education, seeking employment, acquiring financial independence, and moving away from family and home. Many consider these events to be pivotal points in the transition towards adulthood. In the Asian context, these life events tend to occur at later ages. This may be attributed to the traditional Asian values of filial piety and the societal norm of living in a multigenerational household.
According to the various population census [10], there are stark differences in terms of ages at which children move out of the parental home. In Hong Kong, 53% of males and almost 47% of females aged between 15 and 34 lived with their parents in 2015. Around 29% of young adults in Australia live with their parents, according to the 2011 census, up from 21% in 1976. Some 97% of unmarried people aged 15 to 34 lived with their parents in Singapore as of 2013, according to the statistics bureau. For married people, it was 37%.
As such, the Asian adolescent is usually thought to be more reliant on parental influence when making decisions. In the context of IBD care, major decisions such as initiating biologic therapy usually tend to be a shared family decision, especially since there is a financial consideration with regards to the high cost of treatment. Western culture encourages adolescents to move out of the family home and work their way through college with part-time jobs-but it is not the case in the Asian context where most children still rely on their parents to fund their school fees and living expenses until they enter the workforce.
Therefore, it is essential for the multidisciplinary IBD team to approach this issue differently based on the cultural context that the team practices in. Bearing in mind that finances is one of the main factors that young adults are unable to step away from the financial comfort of their parents/caregivers, the psychologist and social worker in charge of the case should actively engage the adolescent early on. As young IBD patients have the tendency to feel dependent a lot of the time as they have always played the role of the ŌĆ£sick child.ŌĆØ Hence, seeking employment and financial independence may not be their priority. It is important for the various stakeholders (such as the IBD nurse, pediatric gastroenterologist and social worker) not to neglect the psychosocial growth of the child as well. However, we must not forget that good control of the underlying disease will lead to better growth of the child and hence less disruption to his/her physical and emotional growth. As such, the child would be able to lead a normal life as much as possible, and be confident in his/her ability to care for and make important medical decisions for themselves. This will subsequently empower them to be mentally and financially self-sufficient, so that the parental role may be reduced.
On the other hand, we should not forget that change can be implemented from the parents/caregiversŌĆÖ side as well. Parents who may potentially be overly protective of their child and hence impede the process of transitioning should be identified early by the healthcare provider so that the multidisciplinary team can make the efforts to effect a change in mindset when the patient is approaching the period of transition. Sometimes, these caregivers may even require emotional counseling from feeling lost after not having a dependent to look after anymore. They may struggle with the sense of wanting to continue taking care of the patient, while on the other hand, wanting the patient to be independent. These feelings may eventually be transferred onto the patient who feels conflicted about wanting to be take charge without negating the appreciation for the parental care that has been provided since childhood. Therefore, the role of the social worker and the psychologist will come in handy in such cases.
We would also like to emphasize that cultures are diverse even amongst various Asian nations. Hence, it is important to individualize each transition program according to each countryŌĆÖs unique culture and values.
BARRIERS TO A SEAMLESS TRANSFER
1. Physician Factors
1) Lack of Knowledge and/or Experience
This is especially so for adult physicians who may not be wellversed in the area of adolescent medicine. As we have described above, many adolescent patients are undergoing major changes in their lives at the proposed age of transition of 18 years. This is an understandably delicate period of change when patients have different physical and psychological needs. Adolescents may be going through periods of experimentation in all areas from recreational drugs to cosmetic procedures, and providers with more in-depth knowledge of the intricacies of medical management in relation to these areas of adolescent medicine would be better able to advise patients and their parents.
A survey amongst Japanese adult gastroenterologists also found that physicians in practice for 30 years or more reported less hesitancy in taking over medical care for childhood-onset patients referred from pediatric gastroenterologists [11]. Hence, the benefit of a team of IBD physicians is that junior physicians are able to continually learn from their more experienced colleagues. This is important as patients and their caregivers need to have confidence in their physician in order to build a trusting relationship that would promote self-efficacy, self-empowerment, and compliance to their medical treatment.
2) Poor Coordination of Care between Adult and Pediatric Providers
This may be largely attributed to the lack of a specialized IBD nurse who also plays the important role of a transition coordinator. The same Japanese survey identified poor coordination of care and inadequate medical summaries as barriers to smooth transition [11].
The lack of coordination of care can sometimes also be attributed to logistical factors such as funding, availability of nursing and allied healthcare support, and the patterns of referrals to tertiary centers. In areas with lower socioeconomic status, these factors may ultimately prove to be the largest barrier to a proper transition program.
2. Patient Factors
1) Poor Health Literacy/Disease-Specific Knowledge
Studies have found that physicians tend to overestimate their patientsŌĆÖ health literacy-related readiness for transition [12]. Hence, validated tools may be used to assess functional and interactive health literacy instead. For example, the Test of Functional Health Literacy in Adults [13] may be used. The 24-item CrohnŌĆÖs and Colitis Knowledge Scale [14] can also be used to assess patientsŌĆÖ interactive health literacy.
2) Lack of Self-Efficacy
The slow uptake of objective evidence-based assessment tools for measurement of patientsŌĆÖ self-efficacy is concerning as physicians may gauge this poorly. In IBD, the most commonly used transition readiness assessment tool is the Transition Readiness Assessment Questionnaire (TRAQ), a 20-item self-report questionnaire regarding disease self-management skills [15]. However, the TRAQ does not take into account the perspectives of the parent/caregiver and/or the healthcare provider. A potential area for further research would be a comprehensive assessment tool that comprises the parentŌĆÖs and providerŌĆÖs gauge of the patientŌĆÖs readiness to transition as well.
3) High Level of Parental/Caregiver Involvement
An Ohio group conducted focus group interviews amongst parents/caregivers and found that majority of parents reported that they were heavily involved in their childŌĆÖs IBD care [16]. This included recognizing when medical care is needed, knowing their childŌĆÖs treatment history, scheduling and attending appointments, answering and asking questions during clinic visits, ordering and picking up refills, and handling financial matters.
The degree of patient independence from their parents/caregivers is crucial in ensuring success for transitional care. The aim is to empower patients with better knowledge about their disease, and also to encourage them to find out more about their condition on their own. This self-empowerment will build a continual cycle of self-interest and a strong desire to seek better control of their IBD. Pediatric gastroenterologists must promote patient independence at regular clinic visits using appropriate tools or programs (e.g., guidelines for autonomy support of patients with IBD in the transitional period [17]. High level of parental involvement may serve as a barrier to the development of youth self-management skills.
3. Disease Factor
The difficult-to-control disease would inevitably draw out the period of transition as it would be difficult to find an opportune time for transition. Challenging diseases may also be contributed in part by the patient/parentŌĆÖs noncompliance to treatment from a young age. These patients would often be labeled as having recalcitrant disease as they are noncompliant to treatment and hence are deemed to have ŌĆ£failedŌĆØ multiple lines of therapy. Therefore, we cannot emphasize more on the importance of setting strong groundwork from the point of diagnosis so as to ensure good patient compliance and understanding of his/her disease.
CONCLUSION
Transitional care is increasingly recognized as a mandatory part of the provision of care in any tertiary IBD center. However, there is a lack of evidence-based data on the ideal proposed transition program. Various objective self-assessment tools measuring health literacy and self-efficacy have been validated in the IBD cohort, and we encourage the use of these tools at specialized transition clinics. In conclusion, we have provided a proposed structure for transition based on the experience at our center, and also highlighted the important points to note especially when treading through the different cultural context in the Asian IBD population.