A massive bleeding from a duodenal mass: what treatment option should be chosen?
Article information
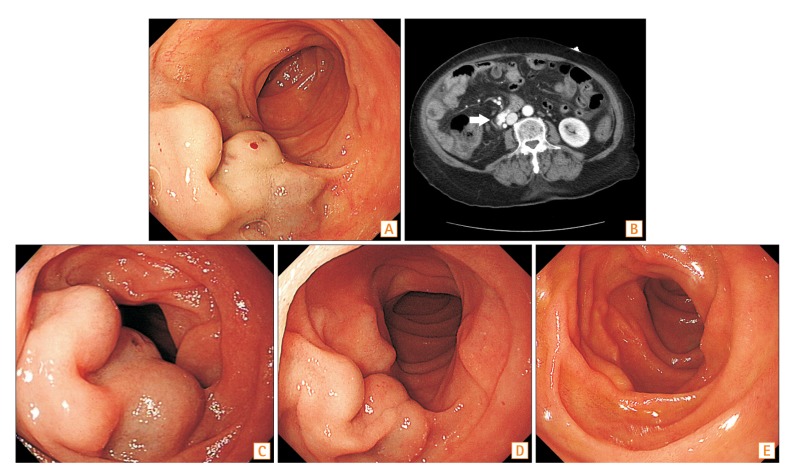
Question: A 78-year-old woman presented with 500 mL hematochezia, hypotension, and a hemoglobin level of 5.4 g/dL. She had a history of right hemilobectomy of the liver and hepatojejunostomy for Klatskin tumor IIIA at other institutions 2 years before. Her medical history also included mitral regurgitation. Emergency esophagogastroduodenoscopy revealed a large, bluish, rugged mass with a smooth surface in the 3rd portion of the duodenum. A red spot was observed at the middle of the lesion (Fig. A). Contrast-enhanced CT of the abdomen revealed a brightly enhanced mass without lobulation in the same location (Fig. B, arrow). What was her diagnosis, and how would you treat the patient?
Answer to the Images: Ectopic Varices in the 3rd Part of the Duodenum
Her diagnosis was duodenal varices. First, endoscopic band ligation of the varices was considered. However, the lesion was too huge to be obliterated completely. Endoscopic sclerotherapy could not be performed because of the risk of lipiodol embolization through a large-bore efferent systemic shunt from the varices. Therefore, the patient underwent angiographic embolization under fluoroscopic guidance, and the lesion was successfully obliterated. Three days after vascular intervention, follow-up endoscopy revealed slight discoloration and reduction of the varices without evidence of bleeding (Fig. C). Further regression of the varix was observed on follow-up endoscopy after 1 week (Fig. D). Finally, the duodenal varix completely disappeared 3 months after the intervention (Fig. E).
Duodenal varices account for 1% to 3% of all portal hypertensive varices.1 The incidence of duodenal varices is relatively rare. However, once it occurs, it can cause life-threatening bleeding.2 Duodenal varices can be treated surgically, endoscopically, or radiologically.3 Recently, cases of successful endoscopic approach for duodenal varices have been reported.4567 However, the possible limitations of an endoscopic procedure should be considered before its application. Failed endoscopic treatment and its complications, such as bleeding from damaged varices or duodenal perforation, often lead to surgery. In this case, old age, cancer history, and deterioration of the general condition due to massive bleeding limited the operation under general anesthesia. Moreover, the patient had a concurrent large ovarian tumor, and its collaterals communicated with the varices. Therefore, complete ligation of the varices with non-endoscopic method was needed.
The patient with a relatively high risk of complication was treated successfully using a non-endoscopic method. Although duodenal varices are difficult to access endoscopically, treatment methods should be chosen with consideration of its risk, even if they are accessible. Fortunately, we could observe the endoscopic progress of the radiologically treated rare presentation of ectopic varices in our patient.
Notes
Financial support: None.
Conflict of interest: None.