.
.INTRODUCTION
Ulcerative colitis (UC) is 1 of the 2 major phenotypes of chronic IBD, which afflicts millions of individuals throughout the world with debilitating symptoms that impair function and quality of life. Further, UC frequently affects women of childbearing age.
Tacrolimus is a calcineurin inhibitor, which inhibits inflammatory cytokine release by activated T-cells. Historically tacrolimus has been known as an immunosuppressant used orally and has shown efficacy in patients undergoing organ transplantation or affected by an autoimmune disease.1 Recently, tacrolimus has found applications in UC patients.2 With this background in mind, we thought that tacrolimus might be an effective medication for UC during pregnancy. However, to our knowledge, hitherto no study has evaluated the safety of tacrolimus in pregnant UC patients or on pregnancy outcome. Here we report a case that experienced a UC flare-up during pregnancy and was successfully treated with tacrolimus and granulomonocytapheresis (GMA) with the Adacolumn.
CASE REPORT
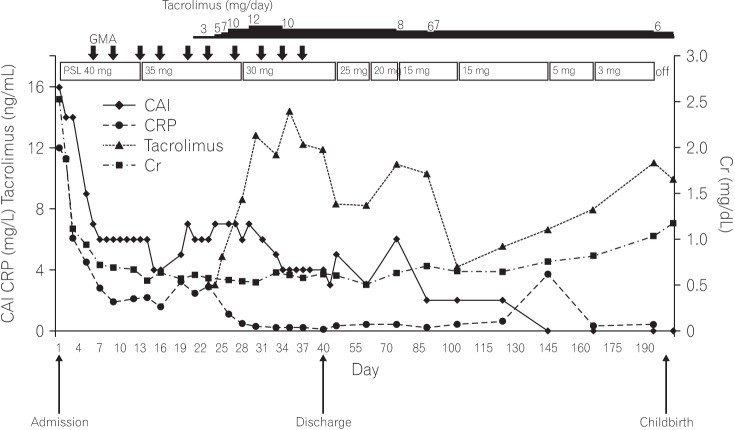
A 38-year-old woman with UC and in the 5th gestational week of pregnancy came to Juntendo Hospital to ask about the risks of UC and the use of medications in general in relation to her pregnancy outcome. Her medical history included a diagnosis of UC (relapse-remitting, total colitis type), which was made 13 years previously. Additionally, she had had serious allergic reactions to mesalazine. She had started treatment with tacrolimus at 4-6 mg/day and prednisolone sodium phosphate solution 3 years previous to this visit. At our hospital, we decided to discontinue tacrolimus administration because her UC clinical activity index (CAI) was 4 (close to remission level). After 1 week, she experienced a relapse with hematochezia and diarrhea (CAI=13). We arranged a conference with an experienced obstetrician after which we re-administered tacrolimus at 6 mg/day. However, due to hyperemesis gravidarum, she could not take any medicine orally and developed dehydration as well as an acute renal disorder. Therefore, tacrolimus was discontinued and she was hospitalized. As shown in the Table 1, the patient's serum creatinine level was 2.53 mg/dL on admission together with severe UC (CAI=16). In hospital, she was administered corticosteroid at 40 mg/day (1 mg/kg, body weight) plus GMA therapy with the Adacolumn, but a full remission was not achieved after 3 weeks (CAI=6). Meanwhile, her renal function recovered following fluid replacement therapy (creatinine, 0.61 mg/dL). Following another consultation with the obstetrician, we re-started tacrolimus at 3 mg/day, gradually increasing the dose to reach a high trough plasma concentration of 10-15 ng/mL, and maintained this dosage for 2 weeks. She achieved a stable remission (CAI=4) and was discharged from hospital. She continued taking tacrolimus, achieving a low trough plasma level of 5-10 ng/mL in an outpatient setting (Fig. 1).
This patient continued oral tacrolimus throughout her pregnancy and was able to discontinue corticosteroid. She delivered electively at 36 weeks and 3 days by cesarean section a healthy baby boy (Apgar score 9/10) with a birth weight of 2,296 g. She was discharged from hospital at postoperative day 5. The baby is now 10 months old and growing well. There is no evidence of any functional impairment or developmental delay.
DISCUSSION
This case with active UC during pregnancy and intolerant to first-line salicylate preparations demonstrates a serious challenge in therapeutic settings. When active IBD develops at the time of conception the disease activity as well as the medical therapy must be viewed as two independent factors that may adversely impact the pregnancy outcome. Indeed, higher relapse rates have been observed in pregnant IBD patients during the first 2 trimesters. This underscores the importance of advising patients to try to conceive during a stable remission.3,4
There are multiple reports on steroids, salicylates, thiopurines, and anti-tumor necrosis factor (anti-TNF) biologics in the treatment of patients with active UC during pregnancy, but there are inadequate reports on tacrolimus and GMA in this setting. For over 9 years, we have been using GMA as a non-drug therapeutic option to treat our regular IBD patients. GMA is effective, but its appropriate use might be overlooked if started after patients are first exposed to multiple drugs and the disease has become severe and refractory to drugs.5,6 Other subgroups in which GMA has shown efficacy include those in whom immunomodulator drugs are ineffective or are not tolerated. GMA has had a good safety profile, and adverse side effects are uncommon and never severe.5,6,7 Nonetheless, to our knowledge, only a few reports are so far available in the literature about the safety and efficacy of GMA for active UC during pregnancy. Takahashi et al.7 used GMA to treat 3 patients who experienced relapse during pregnancy. The number of GMA treatment sessions applied was 5 to 10. All 3 patients achieved remission, 2 with mucosal healing as well. They reported that GMA as a nonpharmacologic treatment was effective and safe. Although 1 of the 3 cases did not respond well to the initial GMA treatment sessions, a moderate dose of prednisolone enhanced the efficacy of GMA, and tapering of the prednisolone dose shortly after remission was not associated with relapse.7 Also our patient responded to GMA, but did not achieve full remission. Because the patient was pregnant, we avoided colonoscopy to assess her UC severity. However, at the time of confirmation of her pregnancy, the patient was in clinical remission (CAI=4). Therefore, we discontinued tacrolimus administration, but soon after the discontinuation she experienced a flare-up. From her clinical records, we were aware that tacrolimus was effective for inducing remission in this patient. Other likely options would have been anti-TNF-α if she had not responded to tacrolimus.
Like cyclosporine, tacrolimus is widely used for the suppression of graft versus host reactions after bone marrow transplantation or to inhibit rejection after solid organ transplantation. Therefore, hitherto data on pregnancy outcome associated with the use of tacrolimus have mainly relied on non-IBD patients. In women who had undergone kidney transplantation, in the pregnancy guidelines, it is recommended to continue immunosuppressive therapy by cyclosporine or tacrolimus.8 However, despite this recommendation,8 in IBD patients, evidence for cyclosporine is limited to a small number of women who experienced severe relapses of UC during pregnancy.9,10,11 Only a single case report on tacrolimus in a pregnant UC patient has been published.12 No obvious congenital malformations were described in infants of pregnant patients who were treated by either cyclosporine or tacrolimus, although some outcomes were complicated by prematurity and low birth weight. However, it is difficult to differentiate the impact of severe disease from an adverse effect of a drug.
In nonpregnant UC patients, tacrolimus was associated with high clinical response without an increased risk of severe adverse events.13 Accordingly, several guidelines now recommend using tacrolimus for steroid-refractory active UC.14,15 However, currently data on the effect of tacrolimus in pregnant patients and pregnancy outcomes are inadequate. Therefore, physicians may advise women to avoid conception during tacrolimus therapy. Further, although tacrolimus readily crosses the maternal-fetal blood barrier,16 there have been reports of many successful pregnancies in those who have had solid organ transplantations with the incidence of congenital abnormalities not higher than in the general population.17,18 In one study, of 100 pregnancies in 84 women treated with tacrolimus, 4 infants had abnormalities, but there was no consistent pattern of anatomical malformation.19 In our UC patient, tacrolimus induced a stable remission with no obvious maternal or fetal complications. Finally, the safety of tacrolimus has not been determined, but its effectiveness in treating active UC indicates that its benefits are greater than potential risks that have been suspected but not confirmed.
In conclusion, our experience in this case suggests that tacrolimus in combination with adsorptive GMA may be a safe and effective treatment option for patients with UC who experience flare-ups during pregnancy. In particular, patients whether or not pregnant who are intolerant to conventional medications could try tacrolimus. However, we strongly believe that future trials with large cohorts of pregnant patients are warranted to determine the optimal regimen and long-term maternal and fetal safety associated with tacrolimus therapy.