Prevention and management of viral hepatitis in inflammatory bowel disease: a clinical practice guideline by the Korean Association for the Study of Intestinal Diseases
Article information
 , Chang Hwan Choi2,*, Jaeyoung Chun3, Heeyoung Lee4, Eun Sun Kim5, Jae Jun Park6, Chan Hyuk Park7, Bo-In Lee8, Yunho Jung9, Dong-Il Park1, Do Young Kim6, Hana Park10, Yoon Tae Jeen,5, IBD Research Group of the Korean Association for the Study of Intestinal Diseases
, Chang Hwan Choi2,*, Jaeyoung Chun3, Heeyoung Lee4, Eun Sun Kim5, Jae Jun Park6, Chan Hyuk Park7, Bo-In Lee8, Yunho Jung9, Dong-Il Park1, Do Young Kim6, Hana Park10, Yoon Tae Jeen,5, IBD Research Group of the Korean Association for the Study of Intestinal DiseasesAbstract
The treatment of inflammatory bowel disease (IBD) has been revolutionized for the last 10 years by the increasing use of immunomodulators and biologics. With immunosuppression of this kind, opportunistic infection is an important safety concern for patients with IBD. In particular, viral hepatitis is determined by the interaction between the virus and the host’s immunity, and the risk of reactivation increases if immunity is compromised by immunosuppression therapy. Parts of Asia, including Korea, still show intermediate endemicity for the hepatitis A virus and hepatitis B virus compared with the United States and Western Europe. Thus, members of IBD research group of the Korean Association for the Study of Intestinal Diseases have produced a guideline on the prevention and management of viral hepatitis in IBD.
INTRODUCTION
The treatment of IBD has been revolutionized over the past decade with the increasing use of immunomodulators and biologics. With immunosuppression of this kind, opportunistic infection becomes a key safety concern in patients with IBD [1]. In particular, the course of viral hepatitis is determined by the interaction between the virus and the host’s immunity. If immunity is compromised by immunosuppression, the risk of reactivation increases, and HBV reactivations in immunosuppressed patients have been associated with hepatic decompensation in a considerable proportion of cases [2,3]. Thus, risk assessment for viral hepatitis is one of the important quality process indicators for the management of IBD patients [4].
In addition, several areas of Asia, including Korea, show intermediate endemicity for the HAV, while HBV shows moderate prevalence compared with United States and Western Europe. Thus, members of the IBD research group of the Korean Association for the Study of Intestinal Diseases (KASID) provide a consensus on the prevention and management of viral hepatitis in IBD.
METHODS
1. Direction
The IBD Research Group of the KASID decided to produce a evidence-based guideline on the prevention and management of viral hepatitis in patients with IBD in April 2018. To establish the guidelines, a committee consisting of 10 gastroenterologists who were members of the KASID, 2 hepatologists and 1 professor of preventive medicine who acted as a methodologist was formed to develop the guidelines. The committee held 10 meetings, with all members in attendance, until the guidelines were completed, with the first meeting taking place on April 2, 2018. The guidelines addressed prevention and management of viral hepatitis in patients with IBD. We focused on prevention and monitoring, and treatment of viral hepatitis are not included in this guideline. The guidelines were generally made by adapting foreign and Korean guidelines on the prevention and management of viral hepatitis in IBD. However, in the case of 3 key questions, no precise recommendations were included in the guidelines, thus new statements were produced by consensus of the professional group.
2. Process of Development
1) Selection of the Key Questions
The key questions were selected among those raised in actual IBD clinic by the committee members. Three of the key questions were accessed by de novo consensus, with the remaining 6 questions being answered by adaptation of previous guidelines.
2) Searching for Source Guidelines
We selected 183 articles that were published between January 1966 and May 2018 by searching the MEDLINE/PubMed and National Guidelines Clearinghouse web sites.
3) Assessment of Guideline Quality and Final Selection
We identified 13 guidelines that were evidence-based, peer reviewed, and either national or international. According to the Appraisal of Guidelines Research and Evaluation II, each guideline was reviewed by 2 committee members for academic integrity and applicability to actual clinical practice. During the development of the current guideline, the 2015 Korean Association for the Study of the Liver (KASL) hepatitis B guidelines were updated as the 2018 KASL hepatitis B guidelines, and we adapted the updated guideline. Finally, all the 13 highly qualified guidelines (Table 1) [2,5-16] were selected, analyzed, and summarized in terms of their evidence and medical recommendations relevant to our guideline.
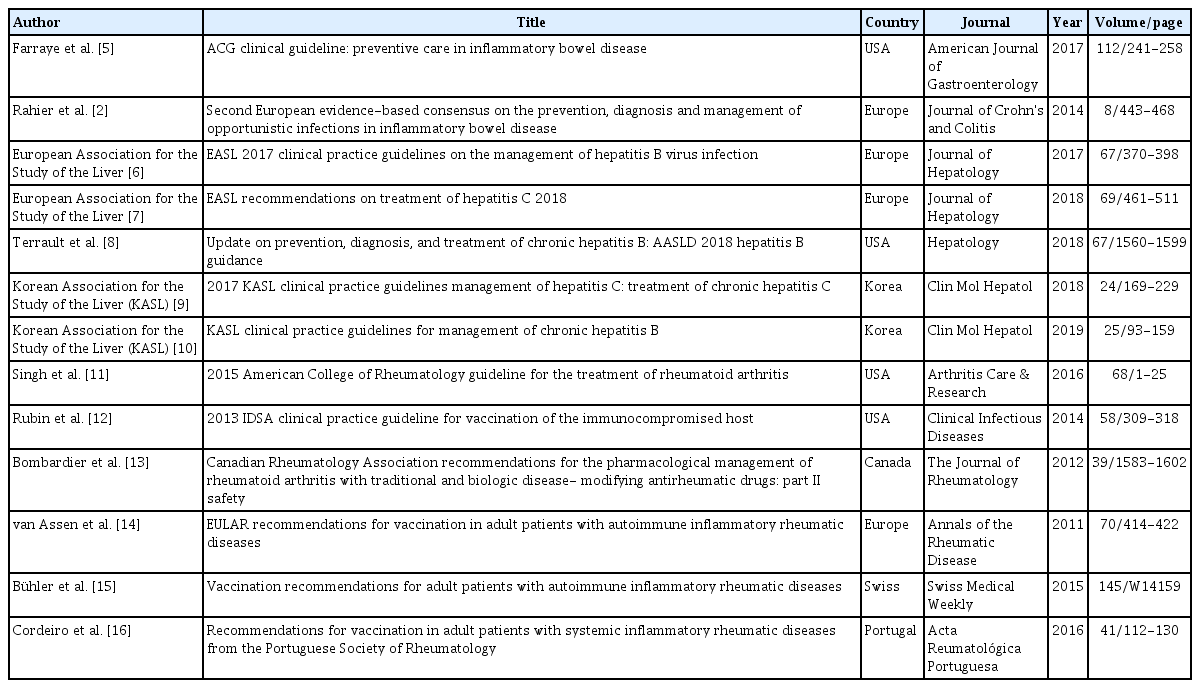
Thirteen Guidelines Selected for Adaptation
4) Adaptation
The evidence and recommendations of the 13 selected guidelines were reviewed, analyzed, and summarized to inform our recommendations and backgrounds. Some of the information therein was deemed to be insufficiently supported by evidence, thus it was discussed in the IBD specialist meetings to be included in the guideline. The quality of the evidence and classification of the recommendations in these guideline are presented by the Grading of Recommendation Assessment, Development, and Evaluation format, by which we assessed the quality of evidence for each recommendation as high, moderate, low, and very low. The strength of each recommendation was classified as strong or weak according to 4 main components: desirable and undesirable effects, quality of evidence, values and preference, and resource allocation. The definition of quality of evidence and classification of the recommendations are shown in Table 2.

Definitions or Implications of the Levels of Evidence and Recommendations
5) Delphi Process for Agreement to Recommendations
On June 14, 2019, the draft of the evidence-based guideline on the prevention and management of viral hepatitis in IBD was presented and proceeded with primary online voting by 40 national IBD specialists who are members of the KASID. The voting participants evaluated each recommendation in the guidelines, stating either strongly agree, agree, uncertain, disagree, or strongly disagree, and the recommendation was adopted when more than 75% of the participants answered strongly agree or agree. The final result was written as a percentage and further classified into levels of agreement.
6) Review, Endorsement, and Distribution of Guidelines
The draft was reviewed and approved by the KASL. The final draft will be published by Intestinal Research and will be provided by the Korean Medical Guideline Information Center (http://www.guideline.or.kr). An updated version is awaiting publication and includes comments by users and newly presented evidence on the prevention and management of viral hepatitis in patients with IBD.
HEPATITIS A VIRUS
1. Epidemiology
The HAV is a small, non-enveloped, single-stranded RNA virus that is transmitted by the fecal-oral route. As such, transmission is increased by poor hygiene, and contaminated food or drink [17,18]. HAV infection is usually a self-limiting illness that does not become chronic, unlike HBV or HCV. Instead, infection confers lifelong immunity and is preventable via vaccination. Furthermore, HAV rarely develops into acute fulminant hepatitis, which can cause death.
HAV infection is prevalent around the world, but it shows various epidemiological patterns that depend on socioeconomic conditions [19,20]. Thus, to adopt appropriate vaccination policies, epidemiologists must ascertain the age-specific antiHAV seroprevalence rates in each country. In highly endemic areas, such as parts of Africa and Asia, the vaccine is not widely used as most adults acquire natural immunity. In areas of intermediate endemicity (such as Central and South America, Eastern Europe, and parts of Asia), childhood transmission is less frequent, while adolescents and adults are more frequently infected, and outbreaks are common. These countries with intermediate endemicity would benefit most from universal immunization of children. In areas of low endemicity (such as the United States and Western Europe), infection is less frequent, but the disease does occur among people in high-risk groups and as communitywide outbreaks. These countries with low endemicity may consider vaccinating high-risk adults.
2. Screening
Statement 1
Patients with IBD should be tested for HAV (IgG anti-HAV antibody) when they have no history of HAV vaccination or HAV hepatitis, or when the history of HAV vaccination is uncertain. In patients with IBD who are negative for the IgG anti-HAV antibody, vaccination should be administered (strong recommendation, very low level of evidence).
· Level of agreement: strongly agree 50%, agree 50%, uncertain 0%, disagree 0%, strongly disagree 0%
Most cases of hepatitis A are directly transmitted through the fecal-oral route, but other propagation paths include indirect transmission through feces-contaminated food or water, blood, or sexual activity. Thus, the Korea Centers for Disease Control and Prevention and the Advisory Committee on Immunization Practices of the United States Centers for Disease Control and Prevention, recommend protection (ideally vaccination) prior to potential hepatitis A exposure in the following high-risk groups [21,22]: those traveling to or working in countries with high or intermediate endemicity of HAV, men who engage in sexual activity with men, users of all illicit drugs, those working with HAV-infected primates or with HAV in a research laboratory, those with chronic liver disease, those with clotting factor disorders, and those in direct contact with others who have hepatitis A.
Patients with IBD are not included in this high-risk group, and their potential for hepatitis A exposure might not different from those without IBD. However, they are often treated with immunomodulators and biologics for long periods, as single agents or in combination, and pre-exposure protection (vaccination) is recommended in immunocompromised patients, as well as in those with chronic liver disease [21].
In HAV, IgG antibodies appear early in the infection phase and remain throughout the patient’s life, preventing disease. The decision to pursue prevaccination serological testing in adults should be based on the expected prevalence of immunity within the given population, as well as on the cost of vaccination compared with the cost of testing. According to rapid economic development in Korea, a rapid epidemiological shift in HAV infection has occurred [20,23]. Most adults had immunity to HAV because of childhood exposure in 1980, but people in their teens or twenties had less than 10% of anti-HAV IgG in 2010 [23]. Thus, the number of adult infected with acute hepatitis A has increased rapidly over the past decade. Since May 2015, HAV vaccination has been recommended for all children between 12 and 23 months in Korea, with high-risk groups being prioritized. Considering the age differences in anti-HAV seroprevalence, the cost of testing, and vaccine prices, those under 30 years of age, who have low HAV antibody rates, are recommended to receive the vaccine without prevaccination serological testing, while those over 40 years of age should undergo a prevaccination serological test and receive the vaccine if the antibody is absent [22].
In patients with IBD, we recommend HAV testing (IgG antiHAV antibody) in patients with no history of HAV vaccination or HAV-related hepatitis, as well as in those whose history of HAV vaccination is uncertain. In patients with IBD who are negative for IgG anti-HAV antibody, vaccination is recommended.
3. Vaccination
Statement 2
HAV vaccination should be administered to patients with IBD using inactivated vaccine, and again at least 6 months later (strong recommendation, with very low level of evidence).
· Level of agreement: strongly agree 35%, agree 55%, uncertain 7.5%, disagree 0%, strongly disagree 2.5%
Hepatitis A is preventable by vaccination. Currently, inactivated HAV vaccines are used as standard vaccination agents and are licensed for administration in a 2-dose schedule given at 6- to 12-month intervals (single dose plus booster dose). Since 1992, 4 interchangeable inactivated monovalent hepatitis A vaccines have become, available which provided protection against all strains of the virus [24]. Protective levels of anti-HAV viruses, persists for at least 20–25 years after vaccination [25]. Although a live, attenuated hepatitis A vaccine is used in some areas because it is cheaper, it has a major disadvantage in that reverse mutation of the live vaccine strains is theoretically possible [26]. Moreover, live vaccines do not offer post-exposure protection because they only illicit a slow immune response [26].
The immune and memory response to the booster dose and the post-booster geometric mean titer, are independent of the interval since initial vaccination [27]. In one study, the effect of the booster on seroprotection was the same across all sexes and age-groups, and the longest time interval between initial dose and booster dose was 11 years, indicating that booster dose can be highly immunogenic for up to 11 years after primary vaccination [27].
Hepatitis A vaccines are safe and highly immunogenic in healthy adults. After 2 vaccinations, with an interval of ≥ 6 months, protective antibody titers reported in > 99% of patients [28-30]. Regarding antibody response according to the number of hepatitis A vaccinations, several studies involving patients with various diseases and medications have reported a significantly higher response after 2 vaccinations than after one vaccination [27,31-33].
Immunosuppressive therapy can lower the antibody response rate of a vaccination. One study including 419 patients with IBD investigated the immunogenicity of the HAV vaccine [34]. Patients were given the HAV vaccine at 0 and 6–12 months, and IgG anti-HAV antibody was measured 1 to 3 months after the second dose [34]. The overall seroconversion rate was 97.6%, but it was significantly lower in patients treated with the antiTNF monoclonal antibody than in those not treated (92.4% vs. 99.1%, respectively; P= 0.001). Furthermore, the seroconversion rate was significantly lower in patients treated with ≥ 2 than with, < 2 immunosuppresants (92.6% vs. 98.4%, P= 0.03). No significant differences in seroconversion rates were seen between patients treated with anti-TNF alone and those treated with anti-TNF plus other immunomodulators (OR, 1.2; 95% CI, 0.2–5.6) [34]. Therefore, the optimal timing to vaccinate patients with IBD against HAV may be at IBD diagnosis, and the vaccine is recommended to be administered prior to immunosuppressive therapy. If HAV vaccines were not available prior to immunosuppressive therapy, it also is recommended to be administered to patients with treated immunosuppression [12].
As the main transmission route of HAV is the fecal-oral route, HAV transmitted through ingestion of contaminated food or drink and causes acute hepatitis [35]. Soon after IBD diagnosis, clinicians should check hepatitis A vaccination history for patients, evaluate their protective antibody status, and carry out vaccination, and again in patients who are planning travel to areas that are highly endemic for HAV, including Southeast Asia, Eastern Europe, and Africa [35]. Patients should also be educated in hand sanitation and cautioned about contaminated food and water.
In general, routine anti-HAV IgG testing is not necessary after vaccination, since the seroconversion rate is very high after the standard 2-dose vaccinations. However, as described above, antibody production after vaccines may be reduced in patients undergoing immunosuppressive therapies, thus measurement of anti-HAV IgG in such patients could be considered 4–6 weeks after a primary course of vaccinations [15]. There are no data on the efficacy and safety of revaccination in patients who are anti-HAV IgG negative after administration of the standard vaccination.
HEPATITIS B VIRUS
1. Epidemiology
The HBV is an infectious disease, with 248 million carriers globally. About 600,000 people die of HBV-related liver disease annually [36]. Although effective vaccination programs are underway, and the rate of new HBV infections has been significantly reduced, HBV is still a major cause of morbidity and mortality.
HBV can be clinically classified as acute and chronic. In the acute phase, the virus may manifest as subacute, non-icteric hepatitis, icteric hepatitis, and sometimes fulminant hepatitis. The chronic phase can be an asymptomatic carrier phase, but it may also manifest as chronic hepatitis, liver cirrhosis, or hepatocellular carcinoma. Both acute and chronic HBV infection may be accompanied by extrahepatic symptoms.
The prevalence of the virus varies by country and region, from 2% in countries with low prevalence (e.g., UK, Canada, Western Europe, etc.), 2%–7% in those with moderate prevalence (e.g., South Korea, Mediterranean countries, Japan, Central Asia, Middle East, and parts of South America), and more than 8% in West Africa and South Sudan, which have the highest prevalence rates [37,38].
In Korea, HBV vaccination of all newborns has been implemented since 1983 (vaccination coverage rate: 79.7%), and the Expanded Program on Immunization (coverage rate: 98.9%) was rolled out in 1995. As a result, Korea is no longer an endemic area, but is classified as having intermediate endemicity [39,40]. In the 1980s, HBsAg-positive carriers comprised 8%–10% of the population. The equivalent rates were 4.6% in the 1990s and 2.9% in 2010. At younger ages, the positive rate of HBsAg was 2.2% in 1998, 1.9% in 2001, and 0.3% in 2016. In IBD patients, the prevalence of chronic HBV infection (positive HBsAg, positive anti-HBc, and negative anti-HBs) was 3.8% and past infection (negative HBsAg, positive anti-HBc, and positive or negative anti-HBs) was 26.2% [41]. The World Health Organization (WHO) has estimated that the prevalence of chronic hepatitis B infection in children under 5 years will be 1% in 2020 and 0.1% in 2030.
2. Screening
Statement 3
All patients with IBD should be tested for HBV (HBsAg, anti-HBs, anti-HBc IgG) at the time of IBD diagnosis. HBV DNA should be quantified in patients with positive HBsAg or anti-HBc IgG (strong recommendation, with high level of evidence).
· Level of agreement: strongly agree 95%, agree 5%, uncertain 0%, disagree 0%, strongly disagree 0%
To the patients in countries with moderate to high prevalence, test for HBV before starting immunosuppressive therapy is recommended [42-44]. Moreover, reactivation of HBV infection, with serious consequences, has been reported in immunosuppressed patients with IBD [45]. Therefore, all patients with IBD should be assessed for HBV infection (HBsAg, anti-HBs, anti-HBc) or immunization status. Patients who are positive for HBsAg, HBeAg, anti-HBe, and HBV DNA should also be evaluated [2], as should HBV infection. Vaccination of the unimmunized patients is recommended, especially before biologic treatments are started [2,12]. The risk of HBV reactivation can be increased in patients who are receiving immunosuppressive therapy (including biologics) and are (1) HBsAg-positive or (2) HBsAg-negative plus anti-HBc positive [42]. In one study, the rate of HBV reactivation during biologic treatments for patients with a rheumatic disease was 12.3% in HBsAg-positive plus anti-HBc positive patients [46], while in another it was 1.7% in HBsAg-positive plus anti-HBc positive and HBsAg-negative plus anti-HBc positive patients [47]. Therefore, both HBsAg and anti-HBc (IgG or total) should be tested. HBV DNA should be quantified in patients scheduled to start immunosuppressive therapy who are either HBsAg-positive or anti-HBc-positive at diagnosis [3].
The role of anti-HBs screening before immunosuppressive therapy remains unclear, and the presence of anti-HBs does not imply prevention of HBV reactivation. However, anti-HBs testing may be helpful for detecting past infection in patients who are HBsAg-negative and anti-HBc-positive. Furthermore, loss of anti-HBs can predict HBV reactivation during surveillance [48-50].
3. Vaccination
Statement 4
HBV vaccination should be administered to IBD patients who have negative serology for HBV (HBsAg, anti-HBc IgG, and anti-HBs negative) with no or unclear HBV vaccination history at the time of IBD diagnosis (strong recommendation, high level of evidence).
· Level of agreement: strongly agree 72.5%, agree 20%, uncertain 5%, disagree 0%, strongly disagree 2.5%
The prevalence of HBV in patients with IBD is not different from that in the general population [51-53]. In all HBV seronegative patients (HBsAg, anti-HBc, and anti-HBs negative) with IBD, regardless of the degree of immunosuppression, HBV vaccination is recommended [2,5]. However, some questions have been raised about whether universal vaccination is necessary in areas with low HBV prevalence [54,55]. The WHO recommended administering the HBV vaccine after birth—in all countries with high, intermediate and low endemicity [56]. Despite these recommendations, the rate of routine HBV vaccination in patients with IBD is not high [53,57], according to a study conducted in Spain involving more than 2,000 patients with IBD, only 12% of patients were administered HBV vaccine [53]. Since HBV infection is relatively common in Korea, specific attention should be given to HBV serology testing and HBV vaccination in patients with IBD.
It is not yet clear whether patients with isolated anti‐HBc positivity (seronegative for both HBsAg and anti‐HBs and seropositive for anti-HBc IgG) require vaccination against HBV. The most common cause of isolated anti-HBc positive cases in areas with high prevalence of hepatitis B, such as Korea, is past HBV infection, where immunization is not necessary, but could be considered in an environment where the risk of exposure to HBV is high [58,59].
HBV vaccines should be administered before starting immunosuppression if feasible, and the inactive vaccine is recommended at least 2 weeks before. As the immune response to vaccination is generally decreased by immunosuppression, patients with IBD should be administered HBV vaccine soon after diagnosis, immunosuppressive therapy is commenced, where possible, especially because the disease follows an unpredictable course and necessitates immunosuppressive therapy [5,12]. According to a meta-analysis based on a random-effects model, the pooled rate of a response to HBV vaccination among patients with IBD was 61% (95% CI, 53%–69%) and no immunosuppressive therapy was predictive of an immune response compared to immunomodulatory (RR, 1.33; 95% CI, 1.08–1.63) or anti-TNF-α (RR, 1.57; 95% CI, 1.19–2.08) therapy [60]. However, in patients who require immunosuppression from the time of diagnosis of IBD, HBV vaccination could be administered with commencement of immunosuppressive drugs.
The standard course of hepatitis B vaccination consists of 3 doses administered at 0, 1, and 6 months, and antibodies are usually produced in more than 90% of general population who vaccinated [61]. This standard vaccination may be ineffective in eliciting seroprotection in the majority of previously unvaccinated patients with IBD, particularly those being treated using immunosuppressive therapy [62-64]. Higher or reinforced doses may be needed to achieve anti-HBs response in immunocompromised patients [42,65]. In previous study involving 148 patients, 41% of those receiving standard cycle of the commercial hepatitis B vaccine at 0, 1, and 6 months attained anti-HBs titers > 10 IU/L, compared with 75% of patients receiving an accelerated double-dose protocol at 0, 1, and 2 months [64]. A study reported that the receiving accelerated double-dose at 0, 1, 2 months followed by revaccination (0, 1, and 2 months) at a double-dose if no adequate response is achieved has demonstrated a higher efficacy than the standard schedule [66].
Statement 5
Patients with IBD require to undergo serology testing 1 to 3 months after administration of the last dose of vaccination to assess whether they require revaccination (weak recommendation, with very low level of evidence).
· Level of agreement: strongly agree 20%, agree 55%, uncertain 20%, disagree 5%, strongly disagree 0%
Generally, immune response to vaccination in patients on immunomodulator monotherapy are not different from controls [66]. Therefore, IBD itself may play a role in the suboptimal response to the HBV vaccine [67]. In patients receiving monotherapy with anti-TNF, some but not all studies have demonstrated a decreased immune response compared with controls or patients on 5-ASAs. The immunogenicity of inactivated vaccines may be preserved when administered on the same day as infusion of the anti-TNF, but it may be reduced when the full immunosuppressive effect of the inhibitor has developed after several weeks. This was observed in patients with rheumatoid arthritis, but patients with ankylosing spondylitis revealed good antibody responses, regardless of the time of infliximab infusion [68]. In patients prescribed both an immunomodulator and anti-TNF agent, the immune response to vaccines is lower than in those on monotherapy with an immunomodulator, anti-TNF, or 5-ASAs [69]. In contrast, vedolizumab which shows gut-selective mechanism does not influence the response to parenterally administered HBV vaccine, but did reduce the response to oral cholera vaccine [70].
In healthy individuals, routine immunity testing after vaccination is not necessary. However, in the patients with IBD, whose treatment depends on immune status, serology testing 1 to 3 months after administration of the last dose are required to assess the need for revaccination [44,56,71].
Statement 6
An additional cycle of revaccination is recommended if seroprotection is not achieved after HBV vaccination in patients with IBD (weak recommendation, with low level of evidence).
· Level of agreement: strongly agree 12.5%, agree 70%, uncertain 17.5%, disagree 0%, strongly disagree 0%
An additional cycle (0, 1, and 6 months) of revaccination is recommended if seroprotection is not achieved. There is some debate about what titer level represents adequate protection against hepatitis B, with some groups recommending titers of anti-HBs above 10 IU/L, and others recommending titers above 100 IU/L [61,72]. According to recently published clinical practice guidelines for hepatitis B in Korea, the level of protective titer of anti-HBs is defined as above 10 IU/L, and if the anti-HBs level is below 10 IU/L in immunosuppressed patients, additional vaccinations are recommended [3]. In nonresponders to HBV vaccination, seroprotection was achieved in 44%–100% after 3 additional doses of revaccination. Considering the costeffectiveness in nonresponders to HBV vaccination, vaccination can be discontinued if anti-HBs ≥ 10 mIU/mL after one month of additional first dose (4th) of administration, however, additional second and third doses (5th and 6th) are administered if anti-HBs < 10 mIU/mL. Then HBV serology testing should be performed 1 to 2 months after completion of vaccinations [73].
Although primary hepatitis B vaccination series is completed and HBV seroprotection is achieved, it is highly likely that patients with IBD, especially those on immunosuppressive therapy, experience loss of seroprotection (anti-HBs level below 10 IU/L) during follow-up. In fact, seroprotection falls by 18% per patient-year in this regard [74]. Therefore, serum antiHBs titers should be monitored in patients with IBD who are receiving immunosuppressive therapy, even if HBV seroprotection is achieved after complete vaccination. Based on expert opinion, anti-HBs should be monitored every 12–24 months, especially in the intermediate- and high-prevalence countries [2,5].
Immunocompromised patients with IBD who have loss of seroprotection during follow-up should be advisable given a single booster dose, and clinicians should consider administering another vaccination series at the regular dose if antiHBs titers fail to rise sufficiently. A booster dose is an extra administration of a vaccine after an earlier (prime) vaccination, which differ from revaccination that requires an entire additional cycle (0, 1, and 6 months) of vaccination. T and B cell immune response to the vaccine booster dose is better preserved than that to primary vaccination, because more memory T and B cells are present, having been induced by the previous dose [75,76]. In one prospective study, a booster dose restored immune response in 76% of pediatric patients with IBD who had lost seroprotection [77]. In cases of HIV-infected children, approximately 30% of patients on antiviral therapy who were vaccinated had no protective titers 3 years after HBV vaccination, but 82% had an anamnestic response to a single booster dose [78]. Thus, a booster dose in patients with IBD on immunosuppressive therapy usually generates protective titers, but antibody responses may be lower than in those without immunosuppressive therapy.
A booster dose may be unnecessary in immunocompetent patients with IBD, even though protective titers of anti-HBs wane during follow-up. Long-term follow-up studies have demonstrated that immune memory persists in immunocompetent individuals, even though anti-HBs levels decline [79].
4. Antiviral Prophylaxis
Statement 7
HBsAg-positive and/or HBV DNA-positive (i.e., those with chronic HBV infection) IBD patients who require moderateto-high risk immunosuppressive therapy should receive antiviral prophylaxis that starts before and continue for at least 6–12 months after the duration of immunosuppression (strong recommendation, with high level of evidence).
· Level of agreement: strongly agree 87.5%, agree 12.5%, uncertain 0%, disagree 0%, strongly disagree 0%
HBV reactivation is defined as active inflammation occurring after inactivity in chronic hepatitis B or after resolution of a past HBV infection. HBV reactivation is classified as follows: (1) exacerbation of chronic HBV infection in patients who are HBsAg-positive, or (2) relapse of past HBV infection in patients who are HBsAg-negative plus anti-HBc-positive [80]. Exacerbation of chronic HBV infection is defined as a more than a 100-fold rise in serum HBV DNA compared to baseline among patients who are HBsAg-positive [3]. Relapse of past HBV infection is detected based on reverse seroconversion (seroreversion) from HBsAg-negativity to HBsAg-positivity, or on the detection of serum HBV DNA in patients who are HBsAg-negative plus anti-HBc-positive [3]. In patients with HBV reactivation, a hepatitis flare-up can occur, which is evidenced demonstrated by a more than 3-fold or 100 IU/L increase in serum ALT compared to baseline [81,82].
The risk of HBV reactivation depends on host factors, virological factors, and type and degree of immunosuppression [83]. The host factors include male sex, older age, cirrhosis, and comorbidity requiring immunosuppressive therapy, such as malignancy and IBD [84,85]. Virological factors comprise high baseline HBV DNA level, HBeAg positivity [86-88], and possibly HBV genotype [89-91]. Clinicians should consider assessing host and virological risk factors to decide whether antiviral prophylaxis should be initiated before starting immunosuppressive therapy. Immunosuppression induces HBV reactivation in up to 50% of patients undergoing organ transplantations or anticancer chemotherapy if antiviral therapy is not administered [2]. HBV reactivation has been also reported in patients with rheumatological diseases or IBD who are receiving anti-TNF, such as infliximab, etanercept, or adalimumab [86,92-96]. In two large, retrospective cohort studies, liver dysfunction occurred in 25%–36% of HBsAg-positive patients with IBD receiving immunosuppressive agents, including corticosteroids, immunomodulators, and anti-TNF, and more than 50% of patients who experienced HBV reactivation had liver failure [45,97]. Importantly, most cases of HBV reactivation developed in patients receiving 2 or more immunosuppressive agents for a long period who were positive for HBV DNA and/or had not undergone antiviral prophylaxis. In contrast, HBV reactivation seems to be extremely rare in HBsAg-negative and anti-HBc-positive patients with IBD [45,51].
The risk of HBV reactivation can be divided into high risk ( ≥ 10%), moderate risk (1%–10%), and low risk ( < 1%) based on the type of immunosuppressive therapy used, which was stratified by HBsAg-positive, or HBsAg-negative plus anti-HBc positive [83,98,99]. Prophylactic therapy with potent oral antiviral agents to treat HBV is highly recommended in patients at high or moderate risk of reactivation. In contrast, close monitoring for HBV reactivation is recommended in patients at low risk of reactivation. The risk of HBV reactivation is listed in Table 3.

Risk of HBV Reactivation Related to Immunosuppressive Therapy for IBD
Long-term moderate-to-high dose corticosteroid therapy (oral prednisone ≥ 10 mg/day over 4 weeks) increases the risk of HBV reactivation in patients who are HBsAg-positive, or HBsAg-negative plus anti-HBc positive [98]. Long-term, low-dose corticosteroid therapy (oral prednisone of less than 10 mg/day over 4 weeks) may also increase the risk of reactivation up to 10% in patients who are HBsAg-positive [99], which necessitates antiviral prophylaxis. In contrast, patients receiving shortterm oral prednisone over 1 week are at low risk of reactivation and do not need antiviral prophylaxis [98]. Immunophilin inhibitors such as cyclosporine and tacrolimus may increase the likelihood of HBV reactivation [100]. However, patients receiving methotrexate, azathioprine or 6-mercaptopurine do not require antiviral prophylaxis because they are at low risk of HBV reactivation [98].
Anti-TNF treatments, such as infliximab and adalimumab, confer a high risk of HBV reactivation—up to 40% in patients who are HBsAg-positive [95,101]. Furthermore, this risk is higher when using infliximab than when using etanercept, which is correlated with potency. TNF-α may regulate the adaptive immune response to HBV infection, and recent evidence has demonstrated that TNF-α and related cytokines may play a crucial role in regulating covalently closed circular DNA and HBV replication [102]. Thus, TNF-α blockade can lead to enhanced HBV replication and subsequent reactivation. Anti-integrins, such as natalizumab, vedolizumab, and ustekinumab, have been associated with a moderate risk of HBV reactivation in patients who are HBsAg-positive [103,104], perhaps because the liver is an immune organ with an active influx and efflux of immune cells [105], so these agents may reduce local immune control of HBV replication in the liver.
In patients who are HBsAg-negative plus anti-HBc-positive, antiviral prophylaxis should be considered on a case-by-case basis, considering comorbidities, prevalence of anti-HBc positivity, and health care resources [5]. However, antiviral prophylaxis is not generally recommended in patients receiving immunosuppressive therapy who are HBsAg-negative plus antiHBc-positive and are at low or moderate risk of HBV reactivation [3,6]. The crucial virological event in patients who are antiHBc-positive is HBsAg reappearance (seroreversion), which is closely associated with hepatitis flare [106]. Therefore, pre-emptive therapy is based upon monitoring of HBsAg, HBV DNA, and ALT during and after immunosuppression in patients who are HBsAg-negative plus anti-HBc-positive, and antiviral prophylaxis should be considered in cases of HBsAg seroreversion and/or detectable HBV DNA, regardless of serum ALT [3,6,8,83].
Antiviral prophylaxis should be initiated in patients who are HBsAg-positive and/or have detectable HBV DNA before starting immunosuppressive therapy—most literature specifies 7 days before [107]. Entecavir and tenofovir are preferred to other antiviral agents, because they have high potency and a high resistance barrier, and because several meta-analyses have associated them with reduced reactivation, hepatitis, and mortality [98,107-109]. The antiviral prophylaxis is recommended to be administered 6 to 12 months after discontinuation of immunosuppression [107], as HBV reactivation beyond 12 months reported, particularly in patients who received rituximab (antiCD20 antibody) [110-112].
5. Monitoring
Statement 8
HBV status should be carefully monitored in patients with IBD who are positive for HBsAg or anti-HBc and treated using immunosuppressive therapy (strong recommendation, high evidence level). In patients who are positive for HBsAg, HBV DNA and ALT levels should be monitored every 3 to 6 months during prophylaxis, and for at least 12 months after cessation of anti-HBV prophylaxis (strong recommendation, low evidence level).
· Level of agreement: strongly agree 47.5%, agree 52.5%, uncertain 0%, disagree 0% strongly disagree 0%
In patients who are HBsAg-negative and anti-HBc positive, HBsAg, HBV DNA, and ALT should be assessed every 2–3 months. Antiviral therapy is recommended when HBV reactivation occurs (strong recommendation, very low evidence level).
· Level of agreement: strongly agree 45%, agree 55%, uncertain 0%, disagree 0%, strongly disagree 0%
In patients who are HBsAg-positive, anti-HBV prophylaxis is recommended independent of serum HBV DNA, and HBV DNA and ALT should be monitored every 3 to 6 months during, and for at least 12 months after anti-HBV prophylaxis, because many HBV reactivations develop after antiviral therapy has been discontinued [113-117].
Patients who are HBsAg-negative plus anti-HBc-positive are at lower risk of HBV reactivation than those who are HBsAgpositive. However, HBV reactivation can also occur in these patients [118], and HBsAg seroreversion is constantly associated with hepatitis flare-ups, even though HBV DNA detection leads to seroreversion and hepatitis in only 50% of cases [106]. These patients should be monitored every 2 to 3 months for increased ALT, HBsAg and changes in HBV DNA, both during and after immunosuppressive therapy. Antiviral treatment should be started in cases of detectable HBV DNA or HBsAg seroreversion [6].
HEPATITIS C VIRUS
1. Epidemiology
The global HCV prevalence is estimated at 2.5% (177.5 million of HCV-infected adults), ranging from 2.9% in Africa and 1.3% in the Americas [119]. In the early 1990s, the prevalence of HCV was reported as 1.7% by enzyme immunoassay method among Korean individuals who underwent health screening program [120]. More recently, a nationwide seroepidemiology study demonstrated that HCV antibody positivity rate in Korea was 0.78% [121]. Additionally, HCV antibody positivity rate tended to increase with age. The rate was 0.34%, 0.41%, 0.60%, 0.80%, 1.53%, and 2.31% in individuals aged 20–29, 30–39, 40–49, 50–59, 60–69, and ≥ 70 years, respectively [121]. A high-risk group for HCV infection includes individuals who inject drugs, patients who undergo dialysis, those with hemophilia or Hansen’s disease, and children born to HCV-positive mothers [119,122]. HCV is typically transmitted parenterally. Sexual, perinatal, and sporadic transmission are reported relatively infrequently [2].
2. Screening
Statement 9
We recommend testing newly diagnosed patients with IBD for IgG anti-HCV antibody. If positive, HCV RNA titer should be checked to confirm HCV infection (strong for recommendation, moderate level of evidence).
· Level of agreement: strongly agree 85%, agree 12.5%, uncertain 2.5%, disagree 0%, strongly disagree 0%
Thanks to recent advancements in medication for HCV, most infections can be cured. In fact, HCV elimination is now an achievable goal, and the WHO has set an ambitious but achievable 2030 elimination target [123]. Although patients with IBD are not a high-risk group for HCV infection, those who are infected with HCV should be treated in the same way as the general population. In addition, patients with IBD are at risk of worsening liver function due to immunosuppressive therapy such as TNF-α inhibitors [124]. Therefore, we recommend that patients with IBD be tested for IgG anti-HCV antibody at the time of IBD diagnosis. When IgG anti-HCV antibody is detected by screening [125], the patients’ HCV RNA titer should be tested to confirm HCV infection [126]. If infection is confirmed, patients should be treated according to the HCV clinical practice guidelines [7]. If possible, HCV infection should be treated before biologic treatments of IBD are initiated. However, if HCV-infected patients with IBD cannot delay their immunosuppressive therapy, their liver function should be monitored closely. In a previous systematic review involving a total of 153 patients with HCV who had been treated using TNF-α inhibitor, mainly for rheumatoid arthritis, worsening HCV infection was identified in only one patient [124]. The benefits of immunosuppressive therapy in patients with IBD who have active disease status likely outweigh the risks of the therapy. However, based on current existing evidence, we cannot recommend simultaneous treatment of IBD (using a TNF-α inhibitor) and HCV infection. Drug-drug interactions between HCV and IBD medications may occur, which may increase drug toxicity or reduce drug efficacy [7].
CONCLUSION
In patients with IBD, opportunistic infection is a key safety concern with the increasing use of immunomodulators and biologics. As HBV reactivation in immunosuppressed patients has been associated with hepatic decompensation in a considerable proportion of cases, clinicians are faced with many challenges in the management of patients with IBD.
As Korea is still an area of intermediate HAV and HBV endemicity, we hope that these guidelines for the prevention and management of viral hepatitis in IBD will prevent hepatitis viral infection and reactivation, and that it will lessen confusion among physicians and researchers.
Notes
FINANCIAL SUPPORT
The authors received no financial support for the research, authorship, and/or publication of this article.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION
Conceptualization: Park DI, Jeen YT. Methodology: Lee H., Writing - original draft: Park SK, Choi CH, Chun J, Kim ES, Park JJ, Park CH, Lee BI, Jung Y. Writing - review and editing: Kim DY, Park H, Jeen YT, Approval of final manuscript: all authors.