Proinflammatory cytokines in irritable bowel syndrome: a comparison with inflammatory bowel disease
Article information

Abstract
Background/Aims
Irritable bowel syndrome (IBS) is a common disease often considered as a functional intestinal disorder. Inflammation in IBS is a quite intriguing theory. The aim of this study was to investigate tumor necrosis factor (TNF)-α, interleukin (IL)-1β and IL-6 expression in inflammatory bowel disease (IBD) patients, IBS patients and normal controls.
Methods
IBS and IBD patients along with normal controls were recruited in the study. In all groups, 2 pinch biopsies were taken at each of 3 anatomical sites (terminal ileum, cecum, and rectum). IBS patients were also subcategorized according to the syndrome clinical manifestations. Two monoclonal antibodies (mAb), TNF-α mAb and IL-6 mAb, and one polyclonal antibody IL-1β mAb were applied for immunohistochemical analysis.
Results
In IBD patients intensity of TNF-α and IL-1β were lower than in IBS patients or controls, while IL-6 was significantly increased comparing to the aforementioned groups. In IBS patients TNF-α was increased comparing to IBD patients or controls, while IL-6 and IL-1β were similar to controls. In IBS subgroups, TNF-α was lower in diarrhea predominant IBS patients and higher constipation predominant IBS patients. Differences among IBS subgroups regarding IL-6 and IL-1β were nonsignificant.
Conclusions
IL-6 seems to be the most important proinflammatory cytokine in IBD patients, while TNF-α could play a more significant role in IBS pathogenesis.
INTRODUCTION
Irritable bowel syndrome (IBS) is a chronic, fluctuating disorder with frequent relapses that affects approximately 20% of adults, accounts for 40% of referrals to gastroenterology clinics, and comprises 12% of general-practitioner consultations [1]. IBS is a disorder without a clear and uniform biochemical, anatomical or pathophysiological substrate. The most prominent symptoms are abdominal pain or abdominal discomfort and an altered defecation pattern. As there are, by definition, no biological parameters for diagnostic discretion in IBS, symptoms constitute a reliable basis for classification and diagnosis. Several acknowledged criteria such as “Manning criteria” followed by the “Kruis criteria” and the “Rome criteria (I-III),” have been used in order to establish diagnosis.
IBS has been considered a common functional disorder implying a disorder without a discernible pathophysiological mechanism, thus a nonorganic disorder [2,3]. Traditionally, IBS has been viewed upon as a disorder where altered GI motility, visceral hypersensitivity, dysregulation of brain-gut axis, altered bowel motility, neurotransmitter imbalances and psychosocial factors are the most important pathophysiological factors [4,5].
The lack of an orchestrator of the IBS mystery is probably the more significant quest regarding the disease. The last few years an emerging theory of inflammation as the key pathophysiological factor in IBS has become quite intruiging [1,6,7].
The aim of this study was to investigate mucosal levels of ΤNF-α, interleukin (IL)-6 and IL-1β in inflamed mucosa (IBD patients), in non-inflamed mucosa (normal controls) as well as in assumed non-inflamed mucosa of patients with IBS.
METHODS
1. Patients
IBS and IBD patients along with normal controls were recruited in the study. Characteristics of IBS and IBD patients and normal controls are described at Table 1. Data regarding IBD patients were mostly retrospective, while IBS patients and controls were recruited prospectively. All subjects underwent colonoscopy after cleansing of their whole colon with polyethylene glycol-electrolyte lavage solution. In all cases, 2 pinch biopsies were taken at each of the 3 anatomical sites (terminal ileum, cecum and rectum). IBD was diagnosed upon clinical end endoscopical criteria as well as by biopsy findings. The endoscopic classification for the IBD group was established using Mayo clinic index and UC endoscopic index for severity [8]. Biopsies obtained from IBD patients with colitis were used as inflammatory disease controls. IBD specimens include patients with CD (CD-terminal ileum), with UC (UC-rectum) and both CD and UC patients (cecum).

Characteristics of IBD Patients, Controls and IBS Subgroups
IBS patients fulfilled the Rome III criteria and none of them had a clear history of IBD. IBS patients were further subcategorized according to their bowel habits (IBS-D, diarrhea predominant IBS; IBS-C, constipation-predominant IBS; IBS-A, patients with alternating symptoms) in order to detect variations in the expression of TNF-α, IL-6, IL-1β in those subgroups. As normal controls were used patients that underwent colonoscopy for polypectomy or investigation of anemia or hematochezia or even patients with colon cancer that had a part of their colon surgically removed (bowel parts remote to cancer margins were used). Controls had: (1) macroscopically and histologically normal colonic mucosa; (2) no persistent bowel symptoms; (3) no organic or functional bowel disease; and (4) no history of chronic medical disease. None of IBD, IBS patients or normal control cases received any anti-inflammatory regimen prior to the time of biopsy.
2. Methods
Tissue specimens were formalin-fixed, embedded in paraffin cubes and 4-μm thick sections were obtained for immunohistochemical study. Immunohistochemical staining was performed on an automated immunostainer (Ventana Benchmark, Strasbourg, France), according to the manufacturer’s protocols.
Antibodies directed against ΤNF-α (dilution 1:100, clone P/T2; Abcam Inc, Cambridge, UK), IL-6 (dilution 1:100, clone 10C12; Leica Biosystems, Wetzlar, Germany) and IL-1β (Thermo Fisher Scientific Inc, Waltham, MA, USA) were applied. Finally, slides were washed in tap water, dehydrated, and mounted with glass coverslips. Positive controls were used to confirm the adequacy of the staining and negative controls were included and consisted in the same immunohistochemical method with omission of the primary antibody.
For the counting of immunopositive TNF-α, IL-6 and IL-1β cells a semiquantitative score system that considered staining intensity on epithelium and crypts was adopted by using the × 40 objective lens and counting at least 5 nonoverlapping fields selected on the basis they contained immunopositive cells. Intensity of TNF-α, IL-6 and IL-1β staining was evaluated as weak (+1), moderate (+2), intense (+3) or severe (+4) on a subjective basis. All immunohistochemical sections were evaluated by 2 independent experienced pathologists. The grade of inflammation was assessed under the same light microscope at × 40 magnification by the same pathologists.
Statistical analysis was performed with SPSS software. Kruskal-Wallis one-way ANOVA test was used to assess the statistical differences between the aforementioned groups. P< 0.05 indicated a statistically significant difference.
3. Ethical Considerations
This study was conducted according to the Ethical Guidelines for Medical and Health Research Involving Human Subjects. The present study was approved by the Ethics Review Committee of University of Ioannina (approval No. 515α/11-11-2003). No additional permissions were required to review the patient records, including the hospitals from which the records were obtained.
RESULTS
1. TNF-α
Intensity of TNF-α was lower in IBD patients through terminal ileum, cecum and rectum, compared to IBS patients and controls (P< 0.05) (Table 2). A nonsignificant increase of TNF-α intensity in IBS patients compared to controls was showed, except at cecum epithelium (P= 0.03).
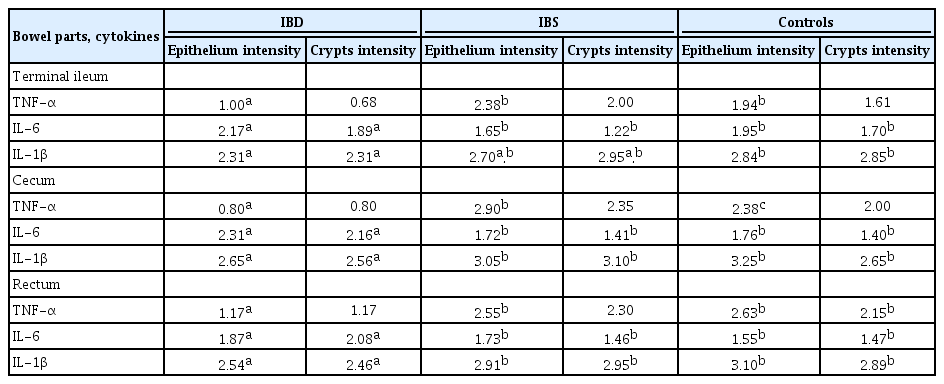
TNF-α, IL-6 and IL-1β in Terminal Ileum, Cecum and Rectum of IBS patients, IBD Patients and Controls
2. IL-6
Intensity of IL-6 appeared higher in IBD patients compared to IBS patients and controls (IBD vs. IBS, P< 0.05) throughout the bowel (Table 2). When comparing expression of IL-6 in IBS patients and controls, no definite pattern was revealed.
3. IL-1β
Intensity of IL-1β was lower in IBD patients compared to IBS patients and controls (IBD vs. controls, P< 0.05; IBD vs. IBS, P< 0,05 at cecum, rectum) (Table 2). Intensity of IL-1β was rather similar in IBS patients and controls.
4. IBS Subgroups
Intensity of TNF-α was lower in IBS-D patients throughout the epithelium and crypts of terminal ileum, cecum and rectum in comparison with IBS-C or IBS-A patients (Table 3). Intensity of TNF-α in IBS-A patients was higher at the rectum and terminal ileum crypts as well as at rectum epithelium (P> 0.05). No statistically significant differences were found in intensity of IL-6 at terminal ileum, cecum and rectum of IBS subgroups, except a significant raise in rectum crypts of IBS-D patients (IBS-D vs. IBS-C/IBS-A, P= 0.001) (Table 3). Finally, intensity of IL-1β was rather similar in all IBS subgroups without significant differences at the terminal ileum, cecum and rectum.
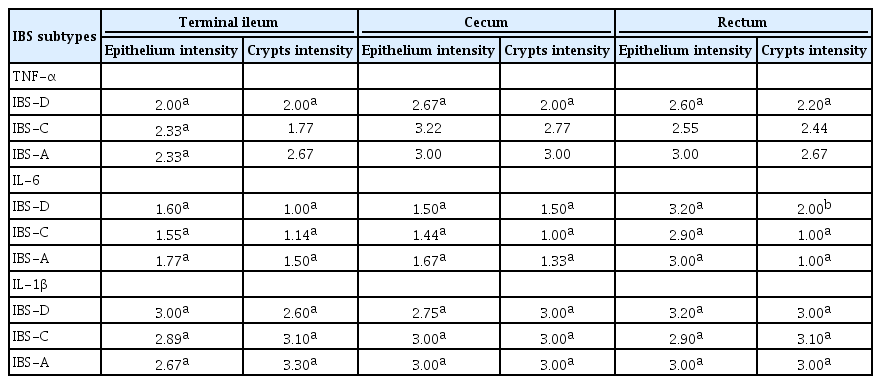
TNF-α, IL-6, IL-1β in Terminal Ileum, Cecum, and Rectum of IBS Subgroups
DISCUSSION
Investigation of pathogenesis in IBDs by analyzing the inflamed mucosa from patients with UC and CD has revealed the increased expression of certain proinflammatory cytokines such as IL-1, IL-6, IL-8, and TNF-α [9]. IL-6 is a pleiotropic cytokine that exerts certain proinflammatory effects and is associated with neoplasia and autoimmune disorders [10]. Stimulation of IL-6 results in a maximal induction of nuclear factor kB (NF-kB) activation and NF-kB nuclear translocation and induces expression of intercellular adhesion molecule 1, an adhesion molecule shown to be important in the neutrophil-epithelial interactions in IBD [11]. IL-6 plays a central role in several immunologic responses during the development of IBD, and circulating levels of IL-6 are associated with many clinical features of CD and UC [12].
IL-6 is expressed in a significantly higher amount in both serum and tissue of patients with active IBD and its levels have been correlated with the severity of the disease and are associated with the prediction of disease activity. T-cell accumulation, mediated by apoptosis resistance, eventually leads to chronic inflammation and can be inhibited by anti-IL-6 receptor antibodies [13,14]. Overall, several studies have highlighted the role of IL-6 in innate and adaptive immune responses and suggest that deregulation of these pathways can contribute to the progression of chronic disease [15].
TNF-α and IL-1β play important roles in the regulation of the immunity, the inflammatory response and the cell growth and death of normal and cancerous cells [16-18]. IL-1 seems to be substantive in the pathogenesis of IBD because of its immunological up-regulatory and proinflammatory activities. IL-1, primarily secreted by monocytes and macrophages, activates intestinal macrophages, neutrophils, fibroblasts, and smoothmuscle cells, inducing them to secrete prostaglandins, proteases, and other soluble mediators of inflammation, and chemotactic cytokines [19].
TNF-α expression in human macrophages was discovered in the colonic tissue and macrophages in both patients with CD and UC and serum levels of TNF-α correlate with clinical and laboratory indices of intestinal disease activity [12]. TNF-α is considered to play an essential role in the pathogenesis of mucosal inflammation in IBD as supported by human and animal studies: (1) in a clinical trial approximately two-thirds of CD patients responded to treatment with a single infusion of anti-TNF-α chimeric monoclonal antibody; (2) amelioration of inflammation following anti-TNF-α treatment in several animal models of intestinal inflammation is presented; (3) the development of a “Crohn’s-like” phenotype in mice that overexpress TNF-α has been shown [9]. TNF-α antibodies have a documented initial effect in 60% to 70% of patients with moderate to severe luminal and/or fistulizing IBD and approximately 30% of patients achieve remission after a relatively short treatment period [20]. Nevertheless, the effect seems to decrease during long-term treatment.
In our study intensity of TNF-α was shown decreased in IBD patients in comparison with IBS patients or controls. Several studies have demonstrated increased mucosal levels of TNF-α in IBD patients [21,22], whereas others were unable to detect increased levels of TNF-α [23,24]. Likewise, the mucosal levels of IL1β were decreased in IBD patients comparing to IBS patients or controls. On the contrary IL-6 mucosal levels were augmented in IBD patients comparing to the aforementioned groups, which corresponds with several studies that place IL-6 as a key factor in IBD [11,25].
Furthermore, it is beguiling that TNF-α mucosal levels were increased in IBS patients in comparison to IBD patients or controls, showing that TNF-α could participate in IBS pathogenesis. Probably, additional research of TNF-α serum levels in IBs patients would provide further data, considering the confirmed elevation in IBD patients, demonstrated in several studies [12]. Levels of IL-6 and IL-1β were similar with those detected in controls revealing possibly a nonsignificant role in IBS. Analyzing IBS subgroups based on symptomatology revealed subtle differences only regarding TNF-α, showing a decrease in IBS-D patients and an increase in IBS-C patients, and no differences in IL-6 and IL-1β in IBS subgroups.
Unprotected elevated levels of TNF-α, IL-6 and IL-1β in controls could be attributable to normal intestinal inflammation [26]. Normal bowel inflammation is a normal response that prevents bowel injury by its ability to fit perfectly into multiple proinflammatory challenges and is therefore essential to homeostasis. The intestine develops and functions within a complex and large microbial load and a steady stream of dietary antigens leading to a “normal inflammation” condition. Anti-inflammatory cytokines such as IL-10 could contribute to diminishing inflammatory procedures in normal controls.
In conclusion, our study demonstrated that IL-6 is probably the most important proinflammatory cytokine in IBD patients, whereas in IBS patients, TNF-α seems a more challenging factor in the disease pathogenesis. Further studies investigating anti-inflammatory or other proinflammatory cytokines in IBS, would provide additional information in the ambiguous pathophysiology mechanisms of IBS as well as the IL-17/Th17 (Thelper 17) axis which is assumed to play an important role in regulating intestinal tissue inflammation [27], and thus, contribute to more effective management.
Notes
FINANCIAL SUPPORT
The authors received no financial support for the research, authorship, and/or publication of this article.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION
Conceptualization: Grammeniatis V. Methodology: Mitselou A, Grammeniatis V, Galani V. Formal analysis: Katsanos K. Project administration: all authors. Writing - original draft: Grammeniatis V, Varouktsi A, Papadatos SS. Writing - review & editing: Mitselou A, Galani V. Approval of final manuscript: all authors