Changes in prevalence and perception of complementary and alternative medicine use in Korean inflammatory bowel disease patients: results of an 8-year follow-up survey
Article information

Abstract
Background/Aims
The use of complementary and alternative medicine (CAM) is a global phenomenon, including inflammatory bowel disease (IBD) patients. We aimed to assess the change in prevalence and patterns of CAM use, and attitudes towards CAM over an 8-year time interval (2006 vs. 2014) among IBD patients in Korea.
Methods
A total of 221 IBD patients (CD=142, UC=79) were asked to complete a questionnaire regarding CAM at two time points: at enrollment (2006) and 8 years later (2014/2015).
Results
The proportion of patients ever using CAM increased significantly from 60.2% in 2006 to 79.6% in 2014 (P<0.001), while the proportion of current CAM users increased slightly (35.7% to 38.0%, P=0.635); 21.7% used CAM consistently at both time points. The proportion of patients who felt CAM was less effective (P<0.001) and more expensive (P=0.04) than conventional treatments increased over time. Also, the proportion among ever CAM users who perceived a positive effect from CAM significantly decreased in 2014 compared to 2006 (P=0.004). Higher education (adjusted odds ratio [aOR], 2.10), prior side effects to conventional therapies (aOR, 2.23), and prior use of corticosteroids (aOR, 2.51) were associated with CAM use. Interestingly, use of CAM before IBD diagnosis (aOR, 2.73) was significantly associated with consistent CAM use.
Conclusions
Although the attitudes toward CAM have become less favorable, the majority of IBD patients have experienced CAM with an overall increase of current CAM users over time. Moreover, more than half of current CAM users used CAM consistently over time.
INTRODUCTION
Complementary and alternative medicine (CAM) includes practices and products of nonmainstream origin that can be used “together with” or “in place” of conventional medicine [1]. In the past two decades, a number of studies investigated the prevalence and patterns of CAM use worldwide [2]. CAM use is now regarded as a global phenomenon, with reports showing 21%–77% of IBD patients using CAM at some point after their diagnosis [2-5]. However, the vast majority of these studies were cross-sectional. Only one study from a population-based cohort of Manitoba investigated the trends of CAM use longitudinally over a period of 4.5 years since 2002 [6]. So far, no study investigated longitudinal data regarding CAM use in the past decade spanning the recent biologic era. Moreover, changes in IBD patients’ perceptions and attitudes toward CAM use over time has not been addressed.
Therefore, we aimed to perform a prospective longitudinal study to determine the changes in the prevalence of CAM use, patterns of CAM use, and the perception and attitude towards CAM between two different time points (2006 and 2014) in a hospital-based IBD cohort in Korea. We further aimed to determine the risk factors associated with previous or current CAM use and consistent CAM use.
METHODS
1. Study Design and Population
The study was based on responses to a questionnaire which was completed at two different time points spanning an 8-year interval by the study participants. Consecutive patients with a confirmed IBD diagnosis who visited the IBD Center at Asan Medical Center, a tertiary hospital in Seoul, South Korea, during November and December 2006 were enrolled upon agreement to participate in the study. The inclusion criteria were as follows: at least 18 years of age at enrollment; at least 1-year of disease duration; informed consent.
At enrollment, study patients were required to complete a questionnaire regarding socio-demographic information (i.e., age, sex, education level, and average income), previous hospitalization or surgery, previous use of corticosteroids or immunomodulators, and the use of different patterns of CAM at the time of survey, during the previous 12 months, or at any time before or after diagnosis of IBD. Additionally, questions regarding the purpose of CAM use, attitude towards CAM in terms of efficacy, cost, and adverse events, and overall confidence in CAM compared to conventional therapy were included in the questionnaire. An English version of the questionnaire can be seen in Supplementary Material 1.
The same questionnaire was completed by the initial participants 8 years after enrollment. The second set of questionnaires were completed between June 2014 and April 2015 among those available to participate. The participants who responded to both questionnaires served as the final samples for the analysis of our study.
The same questionnaire was completed by the initial participants 8 years after enrollment. The second set of questionnaires were completed between June 2014 and April 2015 among those available to participate. The participants who responded to both questionnaires served as the final samples for the analysis of our study.
UC and CD were diagnosed based on the standard clinical, radiological, endoscopic, and histological criteria [7]. Patient demographics and clinical characteristics of IBD, including the date of diagnosis, Montreal classification [8], previous IBD-related surgeries and hospitalizations, and previous medication at enrollment were retrospectively collected from chart review of electronic medical records and from the Asan IBD Registry, which has been prospectively collected and updated since 1997 as described previously [9,10].
Our study was approved by the Institutional Research Board of Asan Medical Center (IRB No. 2014-0920). Written informed consents were obtained.
2. Assessment of CAM Use
CAM was defined in our study according to the National Center for Complementary and Alternative Medicine (NCCAM) in 2005. We used a Korean version of CAM classification which incorporated the 2005 NCCAM classification; CAM was categorized into 7 categories as presented in Table 1. As the NCCAM classification of CAM evolved over time, we reclassified previous categories into CAM products (i.e., herbal therapies, nutrition & diet, folk/traditional medicine, pharmacological and biological therapies) or CAM services (i.e., manipulative and body-based medicine, bioelectronics therapies, mind-body medicine) as described in a previous study6 for further analyses.
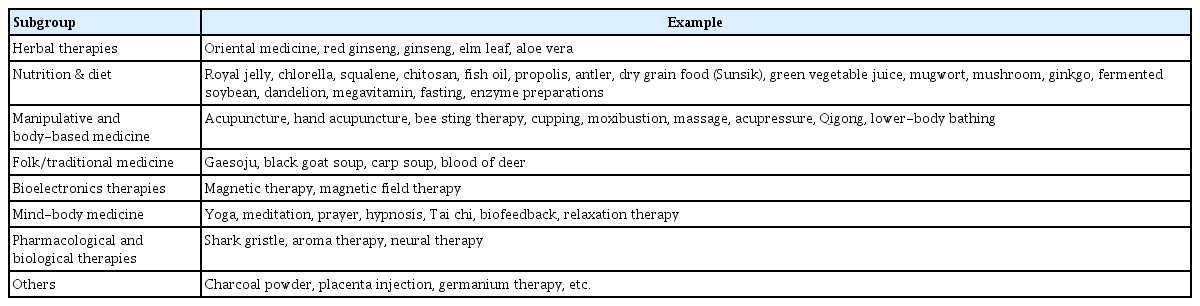
Types of Complementary and Alternative Medicine
3. Definitions of Terms and Study Outcomes
IBD-related hospitalization was defined as at least 48 hours of stay in the hospital due to a flare up of symptoms or other IBD-related complications. Any admission exclusively for the purpose of a diagnostic work up or other conditions unrelated to IBD were excluded. IBD-related surgery was defined as any colectomy in UC patients or any bowel resection in CD patients; of note, surgery due to dysplasia were excluded from this definition. Ever use of CAM was defined as current or previous use of CAM after IBD diagnosis.
The primary outcome of our study was to determine the changes in the prevalence and patterns of CAM use and attitude towards CAM over time in a hospital-based cohort of IBD patients. The secondary outcome was to determine the risk factors associated with ever use of CAM and consistent use of CAM at both time points.
4. Statistical Analysis
Continuous variables were expressed as medians and interquartile ranges, whereas categorical variables were expressed as numbers and percentages. McNemar test was used to compare the paired responses of questionnaires at two different time points. Chi-square test was used to compare the proportion between 2 groups that were considered independent. When comparing the paired results of the questions that had multiple answers, marginal homogeneity test was used. Multivariable logistic regression with backward elimination was used to fit a model for determining risk factors associated with CAM use and to calculate the adjusted odds ratios (aORs) and 95% CI. A P-value of <0.05 was considered statistically significant. Statistical analysis was performed with SAS version 9.4 (SAS Institute, Cary, NC, USA).
RESULTS
1. Baseline Demographics and Characteristics of the Study Participants
A total of 369 IBD patients (161 UC, 208 CD) completed the initial questionnaire in 2006. Among them, 221 patients (79 UC, 142 CD) completed the follow-up questionnaire during 2014 and 2015. Analyses were conducted on the 221 patients who completed the questionnaires at both time points. The baseline demographics and clinical characteristics of the study patients are shown in Table 2.
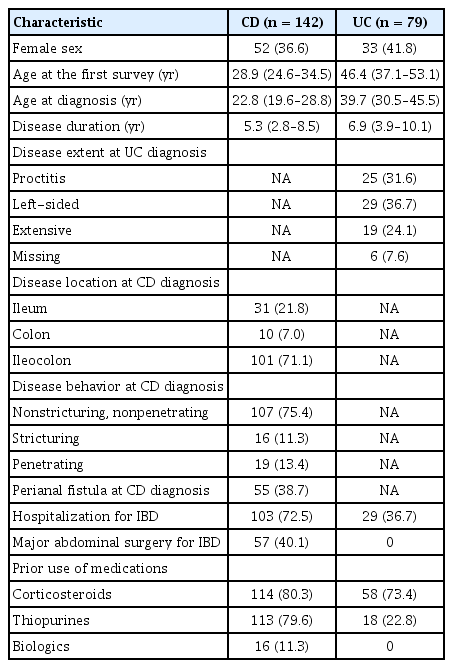
Baseline Demographic and Clinical Characteristics of Study Patients
2. Changes in the Prevalence and Patterns of CAM Use Over Time
The proportion of ever CAM users significantly increased from 60.2% (133/221) in 2006 to 79.6% (176/221) in 2014 (P<0.001). However, the proportion of current CAM users at both time points (35.7% vs. 38.0%, P=0.635) were not significantly different. Notably, 48 patients (21.7%) used CAM consistently at both time points.
The proportion of patients currently using CAM products only, CAM services only, both CAM products and services, or any CAM products or services at the time of survey was similar between time points. The proportion of current CAM users based on the type of disease was similar across time (2006 to 2014: 35.4% to 45.6% in UC, P=0.169; 35.9% to 33.8% in CD, P=0.755). The proportion was also similar across time based on sex (33.1% to 34.6% in male, P=0.878; 40% to 43.5% in female, P=0.690).
The most common types of CAM among ever CAM users based on the follow-up questionnaire in 2014 were herbal therapies (80.7%, 142/176), nutrition and diet (67.0%, 118/176), and manipulative and body-based medicine (27.3%, 48/176). Comparing the types of CAM used within 12 months at each time point, there were no significant differences other than a decrease in herbal therapies in 2014 compared to 2006 (58.8% vs. 75.5%, P=0.014). Among CAM products, red ginseng (59.7%), oriental medicine (50.6%), and fish oil (34.7%) were most commonly used among ever CAM users based on the follow-up questionnaire in 2014.
3. Changes in the Perception and Attitude towards CAM Over Time
Among ever CAM users at both time points (2006, n=133; 2014, n=176), the proportion of patients who perceived a positive effect after using CAM significantly decreased from 45.9% in 2006 to 33% in 2014 (P=0.004).
Attitude towards CAM use in terms of efficacy and cost as compared with that of conventional treatment has changed significantly at both time points. A significantly higher proportion of patients thought that conventional treatment was more effective in 2014 compared to 2006 (62% vs. 44.8%, P<0.001), whereas no significant difference was seen in those who thought CAM was more effective (P=0.219). Also, a significantly higher proportion of patients thought that CAM was more expensive in 2014 compared to 2006 (62% vs. 51.6%, P=0.04).
Regarding the purpose of CAM use, in 2006 the majority of CAM users (50.6%) used CAM to treat IBD, whereas 32.9% used CAM to improve their general health. In 2014, the proportion decreased to 41.7% among CAM users who used CAM to treat IBD, whereas the proportion increased to 41.7% for those aiming to improve their general health; however, the differences in proportions between two time points were not statistically significant (P=0.3 and P=0.3, respectively).
4. Risk Factors Associated with CAM Use
Risk factors associated with ever use of CAM and consistent use of CAM were analyzed, separately. After multivariable analysis, higher education level (aOR, 2.10; 95% CI, 1.05–4.22), prior use of corticosteroids (aOR, 2.51; 95% CI, 1.10–5.76), and adverse events with conventional treatment (aOR, 2.23; 95% CI, 1.08–4.60) were significant risk factors for ever use of CAM. Prior use of CAM before the diagnosis of IBD (aOR, 2.73; 95% CI, 1.35–5.52) was a significant risk factor for consistent use of CAM in the final multivariable model. The results of univariable and multivariable logistic regression of risk factors associated with ever use of CAM and consistent use of CAM are presented in Tables 3 and 4, respectively.
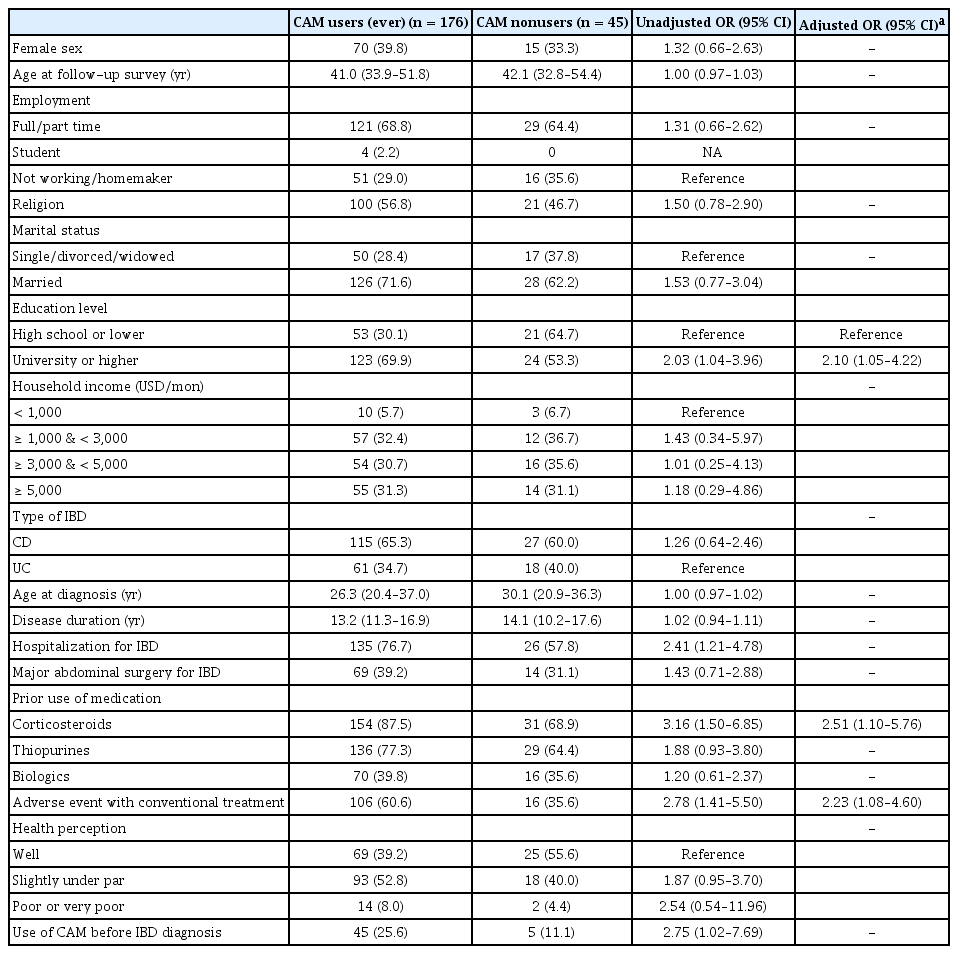
Factors Associated with Ever CAM Use in Patients with IBD

Factors Associated with Consistent CAM use in Patients with IBD
DISCUSSION
In the present study, we sought to investigate changes in prevalence and patterns of CAM use as well as the attitudes towards CAM over an 8-year interval in a hospital-based IBD cohort in Korea. One strength of our study was comparing the responses between both time points from the same initial participants to see if their responses on CAM use have changed over time. Moreover, our study identified predictors for CAM use including predictors for consistent use of CAM at both time points. As the landscape of IBD is ever so dynamic in the past decade in terms of new treatment options and algorithms globally, our longitudinal study may be more reflective of how IBD patients are using CAM during the transition period into the biologic era.
To the best of our knowledge, our study is the first to demonstrate the trend of negative attitudes toward CAM use in the recent years regarding its effectiveness and cost. Our results suggest that significantly more patients feel CAM is less effective and more expensive than conventional treatment compared to about a decade ago. Also, we observed a decreased proportion of those who perceived a positive effect toward CAM among CAM users over the years in the current analysis. However, other factors can potentially influence the results. The availability and approval of more effective therapies including biologic agents for IBD patients may have influenced a relatively positive attitude towards conventional treatment recently [11]. Also, the change of patient environment including the accessibility to medical information from the internet, advent of social media and also activation of on-and-offline IBD communities in the recent years may have influenced our results. Future studies should try to account for the influence of these various factors on the trend of CAM use.
Despite the trend of negative attitude towards CAM across time, the overall proportion of current CAM users slightly increased in 2014 compared to 2006. Also, about 80% of the responders claimed to have used CAM at least once based on the follow questionnaire in 2014. The prevalence of CAM use in the present study is similar to a previous longitudinal study from Manitoba, where 74% of responders used CAM at any time point and about 40% of responders were using CAM at each time point. Interestingly, the proportion of consistent users in our study (21.7%) was similar but slightly higher than what was seen in the Manitoba study (14%) at every time point. Although there was a similar trend of CAM use, the 2 studies were quite different in terms of the patterns of CAM use, the year of which the study was performed, and the type of cohort (hospital-based vs. population-based).
The patterns and types of CAM show a wide variation between cultures and regions. The most common type of CAM used in our study patients at both time points were herbal therapies (predominantly red ginseng) among ever CAM users. This was consistent with a previous Korean study reporting that a quarter of their IBD patients have used red ginseng [12]. In Europe, homeopathy and probiotics are common types of CAM [3,4,13-16], whereas in Canada, probiotics, fish oil, and massage therapy are commonly used among IBD patients [17]. In terms of CAM services, the Manitoba study showed that about 31%–38% of IBD patients use CAM services over time (massage and chiropractic practices were most common in Manitoba) [6], whereas only about 10% of the current CAM users in our study used CAM service at both time points. These variations may reflect a cultural difference or may be caused by a difference in the study methods or classification of CAM as previously suggested by Zezos and Nguyen [2].
Our study investigated risk factors associated with CAM use. Higher education level and previous side effects to conventional treatment were previously reported elsewhere [18-21]. We additionally found prior use of corticosteroids as a significant risk factor in our study. We further looked for risk factors associated with consistent CAM use at both time points; notably, more than half of the current CAM users at each time point used CAM consistently. Interestingly, use of CAM before IBD diagnosis was a significant risk factor. Our results suggest that it is key to ask about the use of CAM even before their diagnosis of IBD, as they may be 2.7 times likely to use CAM consistently over time. Physicians should be aware of these risk factors of CAM use and prepare for proper advice especially in those at risk of using CAM consistently.
Several limitations need to be mentioned. Firstly, a recall bias may have affected our results when answering the questionnaire. Secondly, only about 60% of the initial participants completed the second questionnaire, of whom a better compliance to medical treatment may be expected. As poor compliance to medical treatment could be associated with increased use of CAM [3], the prevalence of CAM in our study may have been underestimated. Thirdly, the generalizability of our results is limited as our study was based on a single referral center. Lastly, we did not account for the change in individuals’ disease activity and the currently used IBD medication over time which may have also influenced the pattern of CAM use and attitude towards CAM.
In conclusion, based on the results of an 8-year follow-up survey, although the attitude toward CAM have become less favorable over time, the majority of IBD patients have experienced CAM with an overall increase of current CAM users over time. Moreover, more than a half of current CAM users tend to use CAM consistently at both time points. Physicians should be aware of the high prevalence of CAM use among IBD patients and prepare for proper advice, especially for those who are at risk of consistent CAM use.
Notes
FINANCIAL SUPPORT
The authors received no financial support for the research, authorship, and/or publication of this article.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION
Study design: Lee SH, Chang K, Park SH. Acquisition of data: Lee SH, Chang K, Seo KS, Cho YK, Song EM, Hwang SW, Park SH, Yang DH, Byeon JS, Myung SJ, Yang SK, Park SH. Statistical analysis and interpretation of data: Lee SH, Chang K, Park SH, Ye BD. Drafting of manuscript: Lee SH. Critical revision and study supervision: Park SH. All the authors approved the final manuscript.
Supplementary Materials
Supplementary materials are available at the Intestinal Research website (https://www.irjournal.org).
Supplementary Material 1.
Study Questionnaire (English Version)