Clinical spectrum of elderly-onset inflammatory bowel disease in India
Article information

Abstract
Background/Aims
Inflammatory bowel disease (IBD) is increasingly being recognized in elderly patients. Data on clinical spectrum of elderly-onset IBD patients is lacking from India.
Methods
A cross-sectional retrospective analysis of a prospectively maintained database of patients diagnosed with IBD was conducted at 2 centers in India. The clinical spectrum of elderly-onset IBD including demographic profile (age and sex), clinical presentation, disease characteristics (disease behavior and severity, extent of disease), and treatment were recorded and compared with adult-onset IBD.
Results
During the study period, 3,922 (3,172 ulcerative colitis [UC] and 750 Crohn’s disease [CD]) patients with IBD were recorded in the database. A total of 186 patients (4.74%; 116 males [62.36%]) had elderly-onset IBD (69.35% UC and 30.64% CD). Diarrhea, blood in stools, nocturnal frequency and pain abdomen were the commonest presentations for UC, whereas pain abdomen, weight loss and diarrhea were the most frequent symptoms in CD. For both elderly onset UC and CD, majority of the patients had moderately severe disease. Left-sided colitis was the commonest disease location in UC. Isolated ileal disease and inflammatory behavior were the most common disease location and behavior, respectively in CD. 5-Aminosalicylates were the commonest prescribed drug for both elderly onset UC and CD. Thiopurines and biologics were used infrequently. Prevalence of colorectal cancer was higher in elderly onset IBD.
Conclusions
Elderly onset IBD is not uncommon in India. Both the elderly onset UC and CD were milder, with no significant differences in disease characteristics (disease extent, location and behavior) when compared to adult-onset IBD. Colorectal cancer was more common in elderly onset IBD.
INTRODUCTION
The aging population and the rise in incidence of inflammatory bowel disease (IBD) across the globe have resulted in increased number of elderly patients with IBD [1]. The cohort of elderly IBD patients includes both patients who have transitioned into older age with IBD having been diagnosed at a younger age (adult-onset IBD) or patients who obtain a diagnosis of IBD at age ≥ 60 years (elderly onset IBD) [2,3]. The elderly IBD patients (including both adult and elderly onset IBD patients) contribute approximately one-fourth of patients to the total disease burden. Of these, nearly 15% of patients have elderly onset IBD [3].
The elderly onset IBD poses unique challenges to the management of IBD owing to concerns like misdiagnosis of IBD due to close mimics like diverticulitis and ischemic colitis, distinct disease behavior, variable efficacy and safety of the medical/surgical therapy due to (in) adequacy of immune response(s) and potential drug interactions due to polypharmacy [3,4]. Additionally, the comorbid illnesses, functional limitations and quality of life are more heterogeneous in elderly patients as compared to their younger counterparts [5]. The gene-environment-microbial interactions also vary with age [6]. Therefore knowledge, awareness and understanding of the age-related differences in clinical course and disease behavior in elderly onset IBD is important to outline a pragmatic approach to the treatment of IBD in this group of patients.
Limited data exists on clinical profile of elderly-onset IBD from Asia, especially India [7-10]. To the best of authors’ knowledge, this is the first focused study reporting the clinical spectrum of elderly-onset IBD from India.
METHODS
1. Study Design
This was a multicenter, retrospective, cross-sectional analysis of patients with IBD enrolled in prospectively maintained medical record databases at 2 tertiary care IBD referral centers in India (Dayanand Medical College and Hospital [DMCH], Ludhiana, north India and Christian Medical College and Hospital [CMCH], Vellore, south India). The database at DMCH Ludhiana was reviewed from January 1, 1991 to December 31, 2020, while at CMCH Vellore, it was reviewed for period between January 1, 2016 and December 31, 2020. The study was approved by institutional ethics committees of both the centers (IEC No. DMCH/R&D/2020/23 and CMCH/IRB No. 12796, respectively). The informed consent was waived.
2. Study Population
The medical record databases of both the participating centers were reviewed. Information on patients with confirmed diagnosis of IBD (established on the basis of Copenhagen diagnostic criteria [clinical, laboratory, radiological, and pathological]) [11,12], visiting the outpatient clinics or admitted in the department of gastroenterology at the participating centers, during the study period, was retrieved.
The details on demographic profile (including age at onset of symptoms, age at diagnosis of IBD, and sex), clinical history (disease diagnosis, clinical presentation, disease characteristics [disease behavior, extent and severity]), medical/surgical treatment and complications were extracted from the databases. Montreal classification was used to assess the disease phenotype in adults with IBD [13]. Disease severity was defined by the Mayo score in patients with ulcerative colitis (UC) and Crohn’s Disease Activity Index (CDAI) in patients with Crohn’s disease (CD) [14,15].
Patients with age at diagnosis between 18 and 59 years were labeled as having adult-onset IBD, while patients diagnosed with IBD at age ≥ 60 years were categorized as having elderly-onset IBD [3]. Pediatric IBD patients (age at diagnosis < 18 years), patients with IBD unclassified and patients with missing data were excluded from analysis.
3. Statistical Analysis
Range, mean (± standard deviation), frequencies (number of cases), and relative frequencies (percentages) were used to describe the data. Quantitative variables were compared using analysis of variance. Categorical data were compared using the chi-square test and the Fischer exact test was performed when the anticipated frequency was less than 5. Probability value (P-value) less than 0.05 was defined as statistical significance. SPSS version 21 (IBM Corp., Armonk, NY, USA) was used for all the statistical calculations.
RESULTS
A total of 3,922 patients with IBD (3,172 UC and 750 CD) were identified from the database and enrolled in the current study (Fig. 1). Out of the enrolled patients, 186 (4.74%) had elderly onset IBD (129 UC [69.35%] and 57 CD [30.64%]), while the remaining 3,736 (95.26%) had adult-onset IBD. There was no significant difference in the proportion of patients with elderly onset IBD in south (CMCH Vellore) and north (DMCH Ludhiana) India (6.88% vs. 4.56%, P=0.06). Majority of the patients in the elderly onset IBD cohort from south India had CD, while UC was predominant in north India (Table 1).
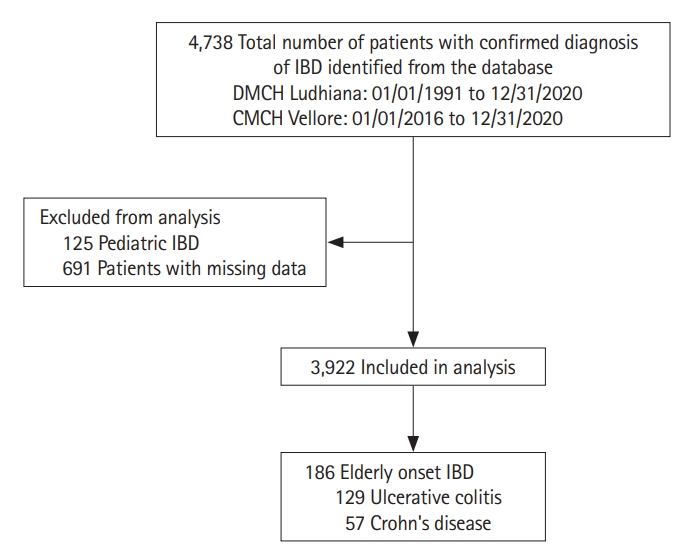
Flow of patients in the current study. DMCH, Dayanand Medical College and Hospital; CMCH, Christian Medical College and Hospital; IBD, inflammatory bowel disease.

Contribution to Elderly Onset Inflammatory Bowel Disease from the Participating Centers
1. Clinical Spectrum of Elderly Onset IBD
The mean age at diagnosis was similar in patients with both CD and UC (68.18 ± 15.70 years vs. 65.88 ± 7.58 years, P=0.17). There was no difference in the mean duration of symptoms before establishment of the diagnosis of IBD. The sex distribution was similar in both elderly onset CD and UC (males 63.15% and 62.01% respectively, P=0.88). A greater proportion of CD patients were smokers (14.03% vs. 7.75%, P=0.18). Only 2 patients (both with elderly onset UC) had positive family history of IBD. Abdominal pain and nausea/vomiting were more common in patients with CD while increased frequency of stools, blood in stools and nocturnal frequency of stools were commoner in UC. Majority of the patients had moderate disease severity (both CD and UC) at the time of diagnosis. Left-sided colitis was the commonest disease extent in elderly onset UC (59.68%) while isolated terminal ileal disease (45.61%) and inflammatory disease behavior (63.15%) were the commonest disease locations and disease behavior, respectively, in patients with CD. Three (5%) patients with elderly onset CD had perianal disease. Nearly one-third patients with elderly onset IBD had extraintestinal manifestations (EIMs); musculoskeletal manifestations (including arthralgias, and peripheral and axial arthritis) being the commonest. 5-Aminosalicylates (5-ASA) were the most commonly prescribed drugs for both elderly onset CD and UC followed by corticosteroids, thiopurines, and biologics. The use of corticosteroids was higher in elderly onset CD as compared to elderly onset UC (68.42% vs. 40.31%, P<0.001). Colorectal cancer (CRC) was more common in elderly onset UC. The mean age at diagnosis of CRC was 67.87 ± 1.88 years. The mean duration of symptoms and duration between diagnosis of IBD and CRC in patients with elderly onset IBD were 7.00 ± 1.06 years and 6.37 ± 1.18 years respectively. Benign intestinal obstruction was more common in elderly onset CD (Table 2).
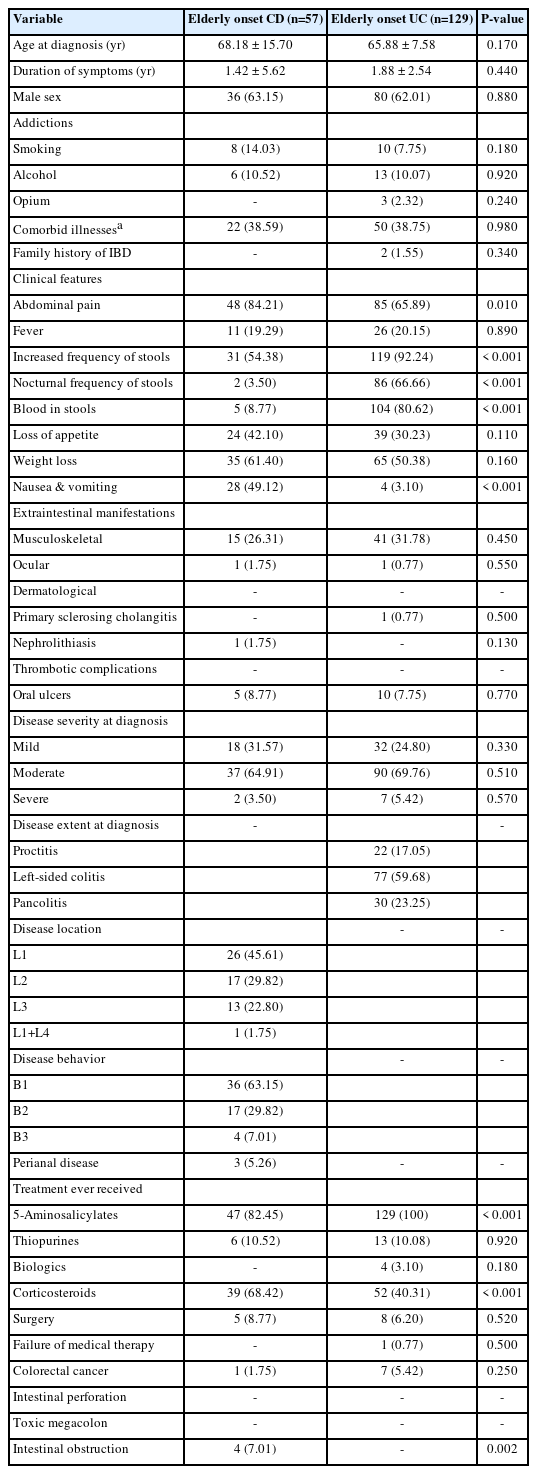
Clinical Spectrum of Elderly Onset IBD
2. Comparison of Elderly Onset IBD with Adult-Onset IBD
1) Ulcerative Colitis
The lag period between onset of symptoms and diagnosis of UC was smaller in elderly onset UC as compared to adult onset UC. Increased frequency of stools, blood in stools, and abdominal pain were the commonest presenting features in both elderly onset and adult onset UC. Increased frequency of stools, weight loss and nocturnal frequency of stools were more common, while loss of appetite was less frequent in elderly onset UC. The disease extent was similar in both the groups, however severe disease was less common in patients with elderly onset UC. Prevalence of comorbid-illnesses, smoking, and musculoskeletal EIMs was higher in elderly onset UC. The use of thiopurines and biologics was infrequent in elderly onset UC as compared to adult onset UC (P<0.001 and P=0.12, respectively). CRC was seen in a greater proportion of patients with elderly onset UC (Table 3).

Comparison of Elderly Onset and Adult Onset IBD
2) Crohn’s Disease
Similar to elderly onset UC, the lag period between onset of symptoms and diagnosis of CD was smaller in elderly onset CD in comparison to adult onset CD. Fever and blood in stools were seen in significantly less number of patients with elderly onset CD. The disease location, behavior, and severity were similar in both the groups, however, the mean CDAI at the time of diagnosis was lower in patients with elderly onset CD. In contrast to UC, there was no difference in the prevalence of EIMs between the 2 groups. Akin to UC, the use of thiopurines was infrequent in elderly onset CD (P<0.001). Biologics were not used in any patient with elderly onset CD. There was no difference in the need for surgical intervention between patients with elderly onset or adult onset CD (Table 3).
DISCUSSION
With the aging global population combined with increased awareness, improved diagnostics and effective therapies, the number of elderly living with IBD has increased. The contribution of genetics, immune responses, and environmental factors in the development of IBD differ across ages [6]. With elderly onset IBD posing unique challenges to disease diagnosis and management, appreciation of the differences in clinical characteristics in patients with elderly onset IBD is important [5,16].
The prevalence of elderly onset IBD in the current study was 4.74%, which is lower than the prevalence reported in Westernized countries as well as in Asia [17-20]. The widely circulated concept of bimodal age distribution of incidence of IBD, could not be appreciated. In industrialized countries, the incidence of elderly onset IBD has been reported to be stable since the 1990s [21-23]. However, there is scarcity of data on the temporal trends from developing countries due to lack of population-based studies. But with the expected epidemiological transition of IBD in India from the stage of acceleration in incidence to the stage of compounding prevalence, the number of patients with elderly onset IBD is likely to increase, mirroring a pattern that was observed in North America and Europe during their epidemiological transitions [24].
In line with previous reports, elderly onset UC was more common than CD [2,25,26]. However regional variations were observed between north and south India. Elderly onset UC was more common in the north, while CD was common in the south. This observation is in agreement with the national IBD survey where CD was reported more frequently in southern India as compared to northern India [27]. Both UC and CD showed predominance in elderly males. These findings are consistent with previous reports of higher frequency of elderly onset UC in males, but differ from earlier observations of elderly onset CD affecting females more commonly [2,6,28]. The higher disease burden of elderly onset CD in males is accordant with reports of overall male predominance in CD in India, across all age groups [29]. This could be due to actual low incidence in females or socio-cultural bias against females in receiving medical care.
The genetic predisposition to IBD is considered an important risk factor for pediatric onset IBD, more than elderly onset IBD. Only 2 patients (both with elderly onset UC) in the current study had positive family history of IBD, highlighting the role of environmental influences and immune responses as the major determinants of disease. Furthermore, age-related physiological changes (including frailty and immunosenescence) and the effect of aging on the intestinal microbiota (shift from anaerobes to facultative anaerobes) also contribute to development of IBD [30]. In the present study, smoking and comorbid illnesses were more frequent in elderly onset IBD as compared to adult-onset IBD. Whether these represent specific differences in the risk factors for adult or elderly onset IBD is not known at the moment and more data are needed to elucidate the pathophysiological differences between the 2 cohorts.
The lag period between onset of symptoms and diagnosis of elderly onset IBD was smaller, as compared to the adult-onset IBD. This is in contrast to the earlier studies where a delayed diagnosis of elderly onset IBD has been reported [31,32]. Early diagnosis of elderly onset IBD after the development of symptoms in the present study can be attributed to the fact that both the participating centers are tertiary care IBD referral centers. This observation, therefore, needs to be interpreted with caution and cannot be generalized as the lag period for IBD diagnosis may be greater in elderly patients reporting to the primary health centers/primary care physicians.
Diarrhea, including nocturnal frequency and rectal bleeding, were the commonest presenting features of elderly onset UC while abdominal pain, weight loss, and diarrhea were the most frequently reported symptoms in elderly onset CD. In comparison to adult onset UC, a greater proportion of patients with elderly onset UC had diarrhea (92.24% vs. 81.13%, P=0.001) and weight loss (50.38% vs. 25.43%, P<0.001), while anorexia was less frequent (30.23% vs. 43.24%, P=0.003). Fever and rectal bleeding were less common in elderly onset CD when compared to adult onset CD (8.77% vs. 31.02%, P<0.004). These observations are in contrast to studies from Western countries where rectal bleeding is reportedly more common in elderly onset CD, but not in elderly onset UC [2,33]. Higher prevalence of rectal bleeding in patients with elderly onset UC and abdominal pain, diarrhea and weight loss in elderly onset CD suggests that Indian patients with elderly onset IBD have a more conspicuous presentation than their Western counterparts. The subtlety of symptoms in elderly onset IBD, as is widely accepted, was not observed in the current study. This may also explain a shorter time to a definitive diagnosis of IBD. The overall prevalence of EIMs was low in elderly onset IBD except musculoskeletal EIMs, which were more common in elderly onset UC.
Left-sided colitis (E2) in UC and isolated terminal ileal disease (L1) were the commonest disease locations. Majority of the patients with elderly onset CD had inflammatory disease. A higher prevalence of isolated colonic inflammation and perianal disease has earlier been reported in elderly onset CD [34-36]. This was not observed in the current study as disease extent/location and behavior were similar in both adult and elderly onset IBD. Differences in diet, genetic makeup and environmental factors might explain the variations in the disease presentation and phenotype [6].
The mean Mayo Clinic score at the time of diagnosis was similar for both adult and elderly onset UC, while CDAI was lower in elderly onset CD. A higher proportion of elderly patients had mild disease in comparison to adult-onset IBD, though the difference was not significant. Severe disease was significantly less common in elderly onset UC.
Overall, 5-ASA were the most commonly prescribed drugs for treatment in both adult and elderly onset IBD due to their perceived safety in the elderly. The use of thiopurines and biologics was expectedly infrequent in elderly onset IBD due to hesitation in their use considering higher risk of adverse effects. Our prescription practices, were comparable to 2 populationbased cohorts from Hungary and France. Both the Hungarian and French cohorts showed that both thiopurines and corticosteroids were more commonly prescribed in adult-onset CD patients compared to the elderly population [23,37]. In the current study, however, despite the risks of infection, insomnia, mood swings, osteoporosis, pathological fractures, and worsening of underlying diabetes mellitus or hypertension in the elderly, the use of corticosteroids was similar in both adult and elderly onset IBD (the use being more frequent in CD as compared to UC). Higher prescription rates of corticosteroids in elderly patients with IBD have also been documented previously [38,39]. Familiarity to corticosteroids, “deemed safety” and hesitation to use immunomodulators and biologics may explain higher frequency of use of corticosteroids.
The need for surgical intervention was similar in both adult and elderly onset IBD groups. The commonest indication for surgery was development of CRC and benign intestinal obstruction (stricturing disease) in elderly onset UC and CD, respectively. The rates of surgery in the elderly onset IBD in the current study were lower as compared to previous reports [40-42]. A recent meta-analysis reported higher surgical rates in the elderly [43]. Lower rates of surgery in the present study indicate either a milder disease course or poor acceptance of surgery in the elderly.
The rate of development of CRC was higher in elderly onset IBD (n = 186; 7 UC and 1 CD, 4.3%) as compared to adult onset IBD (n = 3,736; 21 UC and 2 CD, 0.66%). This observation is at odds with the findings that adult-onset IBD transitioning to elderly IBD is at a greater risk of CRC due to longer duration of disease and persistent inflammation, rather than elderly onset IBD [36,44-46]. Elderly onset IBD, due to supposedly low inflammatory burden and/or a probable different tumor biology, is considered to have a lower risk of CRC. However, significantly high CRC burden was observed in patients with elderly onset IBD (UC > CD). Amongst the elderly onset IBD patients who developed CRC, 2 patients had onset of clinical symptoms before the age of 60 years, but were diagnosed as IBD at > 60 years of age. Therefore, following the definition of elderly onset IBD (age at diagnosis of IBD), these patients were classified as elderly onset IBD, though in true terms they can be considered as adult-onset IBD patients transitioning to elderly IBD. Nevertheless, considering a low overall prevalence of both sporadic CRC and IBD associated CRC in India, the observations of the current study demonstrating a relatively high prevalence of CRC in elderly onset IBD warrants confirmation from well-designed prospective longitudinal studies.
Our study is limited by inclusion of data only from 2 tertiary care centers in India and exclusion of patients with IBD unclassified from the analysis. Also, the understanding of IBD and the clinical care of patients evolved over time. The quality of data captured in the databases during the study period is also expected to have temporal variations. The observations can therefore not be extrapolated as it were. Additionally, as discussed previously, this is a cross-sectional analysis and the patients were not followed longitudinally to discern the natural history and disease course of the elderly onset IBD. A larger population-based longitudinal study is required to understand the true epidemiology of elderly onset IBD in India. The current study however gives a snapshot of the clinical spectrum of elderly onset IBD in India, highlighting the differences in the disease presentation, phenotype, and behavior and complications between India and the Western countries.
In conclusion, elderly onset IBD is less common in India as compared to developed countries, but not rare. Majority of the patients with elderly onset IBD have UC, though regional variations (CD being commoner in south India) are noted. Compared to adult-onset IBD, a higher prevalence of comorbid illnesses and smoking and lower frequency of positive family history was observed in the elderly onset IBD. There were no differences in disease extent/location and behavior between adult and elderly onset IBD. However, there were obvious differences in disease presentation and phenotype when compared to the clinical spectrum of elderly onset IBD in Western countries. Thiopurines and biologics were prescribed rarely in contrast to frequently used 5-ASA compounds and corticosteroids in patients with elderly onset IBD. A higher prevalence of CRC was observed in elderly onset IBD. More studies focused on the elderly are needed to explain the age-related and geographic differences in the disease spectrum of elderly patients with IBD.
Notes
Funding Source
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
Sood A is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Data Availability Statement
Not applicable.
Author Contribution
Conceptualization: Sood A. Data curation: Singh A, Narang V, Singh D, Barnaba Durairaj MV, Dutta AK, Sood A. Formal analysis: Singh A, Narang V, Bansal N, Sood A. Investigation: Singh A. Methodology: Gupta YK, Singh A, Sood A. Project administration: Midha V, Dutta AK, Sood A. Resources: Gupta YK, Singh A, Midha V, Mahajan R, Mehta V, Barnaba Durairaj MV, Dutta AK, Sood A. Supervision: Midha V, Dutta AK, Sood A. Visualization: Singh A, Dutta AK, Sood A. Writing - original draft: Singh A, Narang V. Writing - review & editing: Gupta YK, Singh A, Narang V, Mahajan R, Mehta V, Singh D, Bansal N, Barnaba Durairaj MV, Dutta AK, Sood A. Approval of final manuscript: all authors.