Performing colonoscopy before steroid induction is associated with shorter steroid use in patients with ulcerative colitis
Article information

Abstract
Background/Aims
Risks of long-term steroid use in patients with ulcerative colitis (UC) outweigh the benefits, thus dosing should be tapered once a response is achieved. Colonoscopy is a key technique for assessing disease severity and optimizing treatment involving steroids. This retrospective longitudinal cohort study of patients with UC explored factors associated with the duration of systemic steroid use.
Methods
The Japan Medical Data Center database, an employer-based insurance claims database, was used to select individuals initiating prednisolone, with a prescription issued between January 1, 2010, and January 31, 2018. The study included adults with a confirmed diagnosis of UC, who had received ≥1 year of continuous treatment with 5-aminosalicylic acid, biologics, or thiopurine. Factors associated with prednisolone duration were assessed using a multivariate regression model.
Results
Median duration of prednisolone treatment was 98 days, and colonoscopy was performed ≤1 month before or at the first prescription of prednisolone (index date) in 32.8% of patients (607/1,853). Shorter durations of prednisolone treatment were associated with colonoscopy ≤1 month before or at the index date and higher prednisolone dose at index date, with incidence rate ratios (IRRs) of 0.776 (95% confidence interval [CI], 0.682–0.884; P<0.001) and 0.998 (95% CI, 0.996–1.000; P=0.018), respectively. Charlson Comorbidity Index scores of 1 and ≥2 predicted longer prednisolone treatment (IRR, 1.332; 95% CI, 1.174–1.511; P<0.001 and IRR, 1.599; 95% CI, 1.357–1.885; P<0.001, respectively).
Conclusions
Performing colonoscopy before or at the time of initiating steroid was associated with a shorter duration of steroid use in patients with UC.
INTRODUCTION
Ulcerative colitis (UC) is an inflammatory bowel disease characterized by erosions and/or ulcerations in the mucosal surface of the large intestine [1-3]. Although the prevalence of UC is lower in Japan than in Western countries, it has been steadily increasing over the past few decades [4,5]. For instance, prevalence has increased almost tenfold from 18.1 to 172.9 per 100,000 persons between 1991 and 2014 [6,7].
The current standard-of-care for UC involves a treat-to-target approach, for which patients are regularly assessed to ensure that they are meeting disease control criteria [2,8]. Colonoscopy is a key component of this approach because it helps determine the extent and severity of UC, and helps guide the treatment strategy to achieve remission [1,3,8-10]. For instance, Japanese guidelines [1,3] and other recommendations [9,11,12] state that colonoscopy should be regularly used to assess treatment response and improve disease management in patients with UC. Available treatments for UC consist of 5-aminosalicylic acid (5-ASA), immunomodulators, steroids, tofacitinib, and biologic therapies including vedolizumab, ustekinumab, and anti-tumor necrosis factor-α agents. For mild to moderate disease, 5-ASA is the recommended induction treatment, but steroids are included when the disease is severe or when there is no response to 5-ASA. Steroids are also used in response to moderate or severe flares of UC [1-3,13]. However, steroids are not effective at maintaining remission, which is usually achieved with 5-ASA, immunomodulators, or biologics [1,3,13,14].
Although a high proportion of patients respond to their first course of steroids, over 20% develop dependency in the first year of treatment owing to the pathophysiology of UC [15,16]. Furthermore, physicians may prescribe steroids for extended durations, even though prolonged use is not recommended due to its association with significant adverse events like venous thromboembolism, osteoporosis, and infection [17]. In response to issues of dependence and prolonged use when using steroids, guidelines suggest that doses should be tapered over 8 to 12 weeks following a response [13,14]. Additionally, steroidsparing therapy with immunomodulators or biological agents may improve disease outcomes and reduce complications associated with long-term steroid use.18-20 Nevertheless, prolonged use of steroids and steroid dependence are common among patients with UC in the United States [17] and United Kingdom [21], (also in Japan) even though their use has decreased with the rising use of thiopurines and biologics [22]. Endoscopic severity inversely correlates with the efficacy of steroids, further suggesting the important role of colonoscopy in optimizing UC treatment [10].
In this claims database study, we explored factors associated with the duration of steroid use in patients with UC, with special attention to the effect of performing colonoscopy within 1 month before starting steroid treatment, as per guidelines. Specifically, we hypothesized that performing colonoscopy ≤ 1 month before initiating systemic steroids would be associated with a reduced duration of steroid use.
METHODS
1. Statement of Ethics
The study was conducted according to the Declaration of Helsinki and the International Society for Pharmacoepidemiology guidelines for good practice. It was carried out retrospectively using a database of anonymized data, following ethical guidelines for medical and health research involving human subjects issued by the Japanese Ministry of Health, Labour, and Welfare (https://www.mhlw.go.jp/file/06-Seisakujouhou-10600000-Daijinkanboukouseikagakuka/0000080278.pdf ; accessed April 1, 2021). Institutional ethics approval and informed consent were not required because only anonymized information was extracted from the source database. All authors had full access to the data and take responsibility for data integrity and analysis.
2. Data Sources
This study was conducted using the Japan Medical Data Center (JMDC) database, an employer-based insurance claims database. The database contains monthly claims data submitted to health insurance societies from participating medical institutions and pharmacies since 2005. At the end of 2018, the database contained records of 5.6 million individuals. Claims between January 1, 2010, and January 31, 2018, were included in this analysis.
Individual, anonymized data on sociodemographic characteristics (e.g., sex, age, date of death) and medical claims (e.g., dispensed drugs with date of delivery, laboratory tests, outpatient/inpatient medical care, procedures) were retrieved from the JMDC database. Serious diagnoses were encoded in the database as International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) codes, and were extracted along with the date of disease onset.
3. Study Population
Patients who received daily dosages of the steroid prednisolone, ranging from 1–100 mg/day, through oral (1 mg, 2.5 mg, 5 mg tablets) or intravenous (IV) (10 mg, 20 mg, 50 mg infusions) prescriptions were included in the analysis (Fig. 1). The daily dosage was calculated as the prescribed unit amount × number of doses prescribed per day. The index date was defined as the date of the first prednisolone prescription during the study period. Key inclusion criteria were: age ≥ 18 years at the index date; a confirmed diagnosis of UC at or before the index date (according to ICD-10 code K51); ≥ 1 year of continuous treatment with 5-ASA, adalimumab, infliximab, golimumab, or thiopurine (treatments available for UC in Japan during the study period); no history of colectomy. Patients also needed to have records that extended ≥ 3 months both before and after the index date to be included because treatment guidelines recommend tapering steroid dose over an 8 to 12-week period following treatment response [1].

Flowchart of patient disposition. aPatients can be excluded due to several reasons, therefore sum of excluded patients is over the total number of excluded patients. UC, ulcerative colitis; 5-ASA, 5-aminosalicylic acid.
4. Outcomes
The duration of prednisolone use up to the first discontinuation was the main outcome of interest. For each patient, the JMDC provides an entry for each prednisolone prescription and the number of days it was prescribed. We calculated the median and 90th percentile of days prescribed within each subject, and imputed the median days prescribed for entries that had missing or spurious values (< 7 days). The first discontinuation was determined when the duration between the end of one prescription and the start of the next was greater than the 90th percentile of days prescribed, or if no other prednisolone prescriptions were observed in the record.
5. Exposure to Treatment
Patients were classified into 2 exposure groups based on the duration of prednisolone use (from the first prednisolone prescription up to the first discontinuation): group A, continuous prednisolone use for < 3 months; group B, continuous prednisolone use for ≥ 3 months. This cutoff was based on guidelines that state prednisolone should be withdrawn around 3 months after administration [3].
6. Statistical Analysis
All analyses were conducted at the patient level. Descriptive analyses were performed for the entire patient cohort according to exposure groups (groups A and B). Continuous variables were summarized by group as means with standard deviations, and medians with lower and upper quartiles (Q1–Q3). Categorical variables were treated as frequencies and proportions. Student t-tests or Wilcoxon tests (when variables had nonnormal distributions) were used to compare continuous variables between groups, while chi-square or Fisher exact test (if > 20% of subcategories had expected frequencies < 5) were used for comparing categorical variables.
Several generalized linear models were used to assess factors associated with the duration of prednisolone treatment (number of days from index to first discontinuation; continuous), with each model using a different assumed distribution for the response (negative binomial with log-link, Poisson with log-link, Gaussian with identity link). We restricted our analytical sample to only those patients with complete prescription periods within the observation period. The analytical model was chosen by comparing the goodness-of-fit for each test based on the Akaike Information Criterion (AIC) and the Bayesian Information Criterion (BIC). Covariates used in the regression analyses were: demographics at the index date (sex, age [continuous]); use of an immunomodulator (azathioprine, 6-mercaptopurine) ≤ 3 months after the index date; use of a biologic (adalimumab, infliximab, golimumab [vedolizumab was not approved until July 2018]) ≤ 3 months after the index date; mean number of physician visits per year, calculated based on the number of outpatient procedures recorded on different dates; colonoscopy ≤ 1 month before or at the index date (yes/no); Charlson Comorbidity Index (CCI) score of 0, 1, or ≥ 2 (diagnoses of disease were checked in the 3-month pre-index period); prednisolone dose at the index date (continuous; in the case of severe outliers, a value of 200 mg/day was imputed); history of hospitalization, defined as the number of hospitalizations ≤ 3 months before the index date. Patients that were still receiving prednisolone treatment by the cutoff date were excluded from the dataset to avoid biases associated with observation time (i.e., only patients with an observed discontinuation were included). We repeated this multivariate regression analysis on a sub-group comprising patients that underwent colonoscopy within 1 month before or at the index date.
All analyses were performed using the SAS/STAT software, version 9.4 (SAS Institute Inc., Cary, NC, USA). A P-value of < 0.05 was considered statistically significant.
RESULTS
1. Patients
Between January 1, 2010, and January 31, 2018, 8,030 patients with a prescription of steroids were identified, of whom 4,732 were prescribed prednisolone. After excluding 2,879 patients who did not meet inclusion criteria, 1,853 patients with UC and a prescription for prednisolone were included in the study (shown in Fig. 1). Group A consisted of 887 patients (47.9%) continuously treated with prednisolone for < 3 months and group B consisted of 966 patients (52.1%) continuously treated with prednisolone for ≥ 3 months. The mean age at index date was 40.5 years, and 64.7% of patients were male (Table 1).

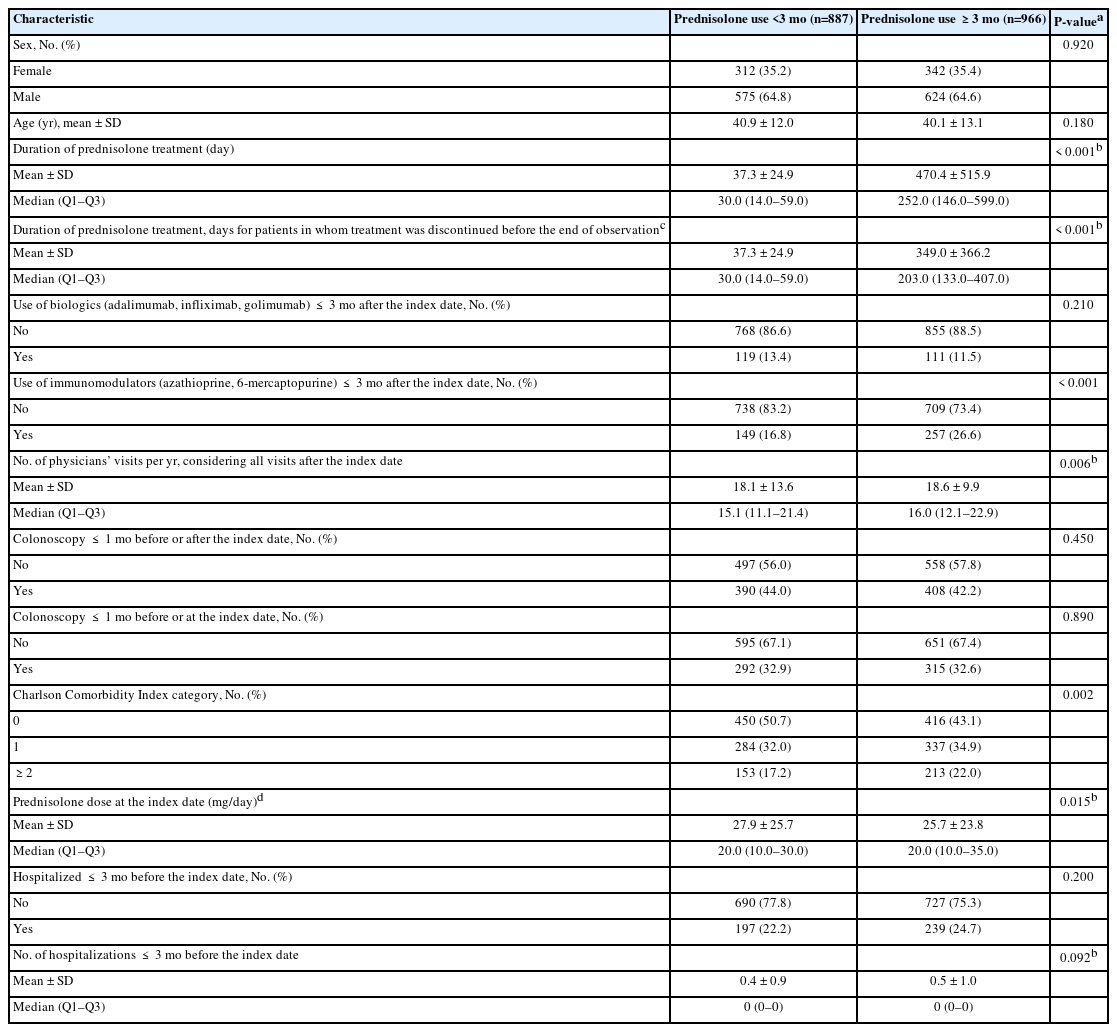
Patient Characteristics
2. Outcomes
The median duration of prednisolone treatment for all patients was 98.0 days (Q1–Q3: 33.0–266.0 days) (Table 1). Overall, 230 patients (12.4%) had used biologics within 3 months after the index date, and 406 (21.9%) had used immunomodulators within 3 months after the index date. The median number of physician visits per year across all patients was 16.0 (Q1–Q3: 11.5–22.2). The median prednisolone dose at the index date was 20.0 mg/day (Q1–Q3: 10.0–30.0 mg/day) and the mean ± standard deviation was 26.8 ± 24.7 mg/day (Table 1, Fig. 2A). Because this value was lower than guideline-recommended doses for UC (30–40 mg/day oral, 40–80 mg/day IV) [1,3], we conducted a post-hoc exploration to determine if the low initial dose rates were related to steroid treatment for comorbid conditions. After excluding all patients with ICD-10 codes other than K51 (UC) within 3 months of index (n = 1,812), the median initial prednisolone dose remained at 20.0 mg/day (Q1–Q3: 10.0–30.0 mg/day), with a mean ± standard deviation at 21.7 ± 11.7 (Fig. 2B). Moving on, colonoscopy was performed ≤ 1 month after the index date in 191 patients (10.3%) and ≤ 1 month before or at the index date in 607 patients (32.8%) (Table 1). Henceforth the analysis is restricted only to those receiving colonoscopy before or at the index date to avoid confounding between different types of colonoscopy.
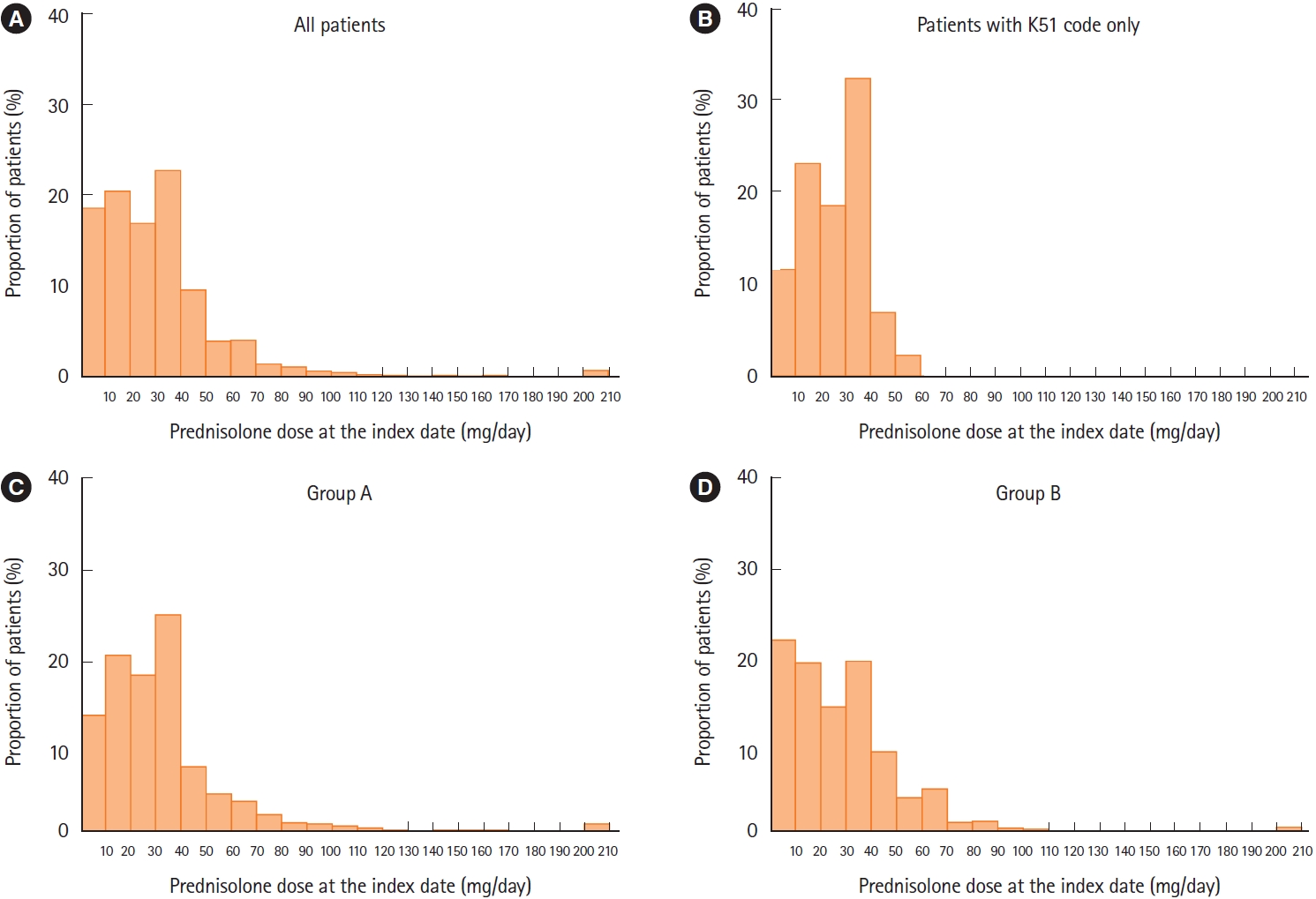
Histograms of prednisolone dose at index date (mg/day) for: (A) all patients (n=1,853); (B) patients without comorbidities (excluding all cases with ICD-10 codes other than K51 [ulcerative colitis] ≤3 months from index; n=41); (C) group A (continuous prednisolone use for <3 months; n=887); (D) group B (continuous prednisolone use for ≥3 months; n=966). ICD-10, International Statistical Classification of Diseases and Related Health Problems, Tenth Revision.
A univariate test revealed no significant association between colonoscopy ≤ 1 month before index and classification into groups A or B (Table 2). However, those treated with prednisolone for < 3 months (group A) received significantly greater dosages at index compared to those treated for ≥ 3 months (group B) according to a Wilcoxon test (Table 2, Fig. 2C and D). Patients in group A were also less likely to have received an immunomodulator ≤ 3 months after the index date and had fewer physician visits per year (Table 2). CCI scores tended to be lower in group A than in group B (Table 2).
Patient Characteristics According to Length of Exposure to Prednisolone
A generalized linear model that assumed a negative binomial distribution and logarithmic link function was selected for the multivariate analysis (AIC negative binomial = 20,616.8, ΔAIC Gaussian = –3,150.6, ΔAIC Poisson = –438,699.2; BIC negative binomial = 20,681.9, ΔBIC Gaussian = 3,150.5, ΔBIC Poisson = –438,694.1). The multivariate regression analysis revealed 4 factors independently associated with prednisolone treatment duration: age at the index date, colonoscopy ≤ 1 month before or at the index date, prednisolone dose at the index date, and higher CCI score (shown in Fig. 3). Duration of steroid use decreased with age at a rate of 0.995 per year of age (95% confidence interval [CI], 0.990–1.000). Colonoscopy ≤ 1 month before or at the index date was predictive of shorter prednisolone treatment duration (incidence rate ratio [IRR], 0.776; 95% CI, 0.682–0.884; P< 0.001). Likewise, a higher prednisolone dose at the index date was also predictive of shorter treatment duration (IRR, 0.998; 95% CI, 0.996–1.000; P= 0.018). Compared with a CCI score of 0, a score of 1 or ≥ 2 was associated with longer prednisolone treatment duration (IRR, 1.332; 95% CI, 1.174–1.511; P< 0.001 and IRR, 1.599; 95% CI, 1.357–1.885; P< 0.001, respectively).
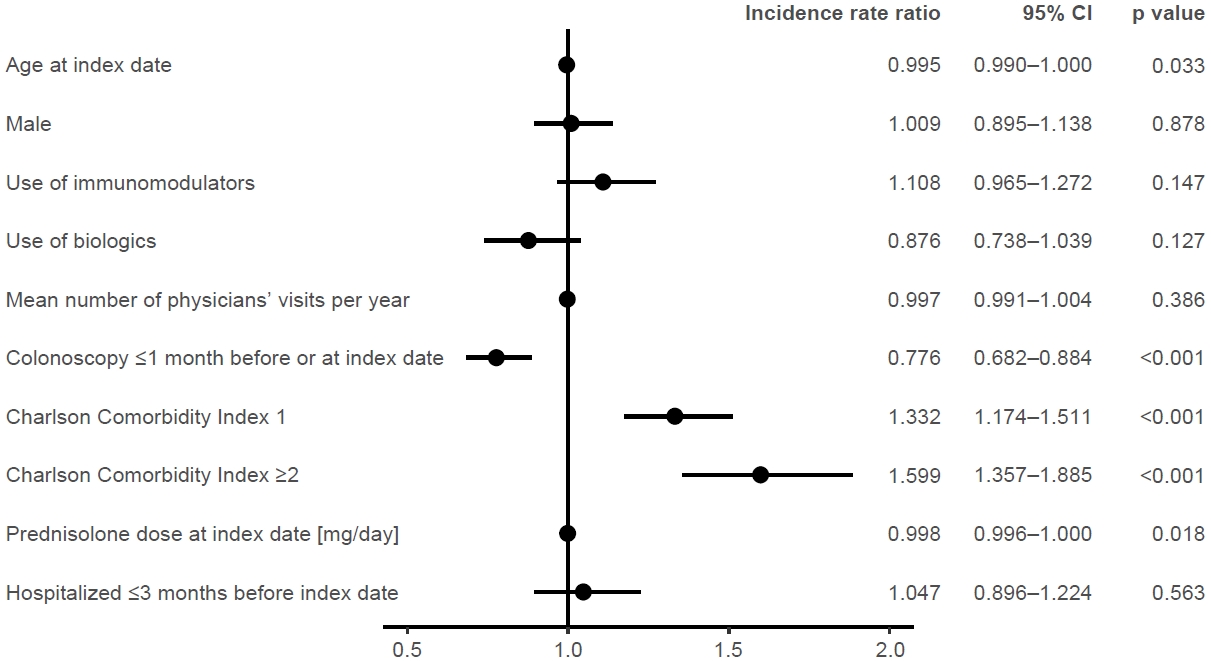
Multivariate regression analyses for association between patient characteristics and prednisolone treatment duration (n=1,673). CI, confidence interval.
The same multivariate regression model was applied to a sub-group of 571 patients receiving colonoscopy ≤ 1 month before or at the index date. This analysis revealed that prednisolone treatment duration was significantly related to sex, use of biologics, CCI, and a history of hospitalization within 3 months before the index date (Fig. 4). Specifically, prednisolone duration was significantly longer in males (IRR, 1.214; 95% CI, 1.014–1.454; P= 0.035), those with CCI ≥ 2 (IRR, 1.497; 95% CI, 1.169–1.918; P= 0.001), and those with a recent history of hospitalization (IRR, 1.220; 95% CI, 1.018–1.463; P= 0.031). Prednisolone duration was significantly shorter in those using biologics (IRR, 0.710; 95% CI, 0.558–0.902; P= 0.005).
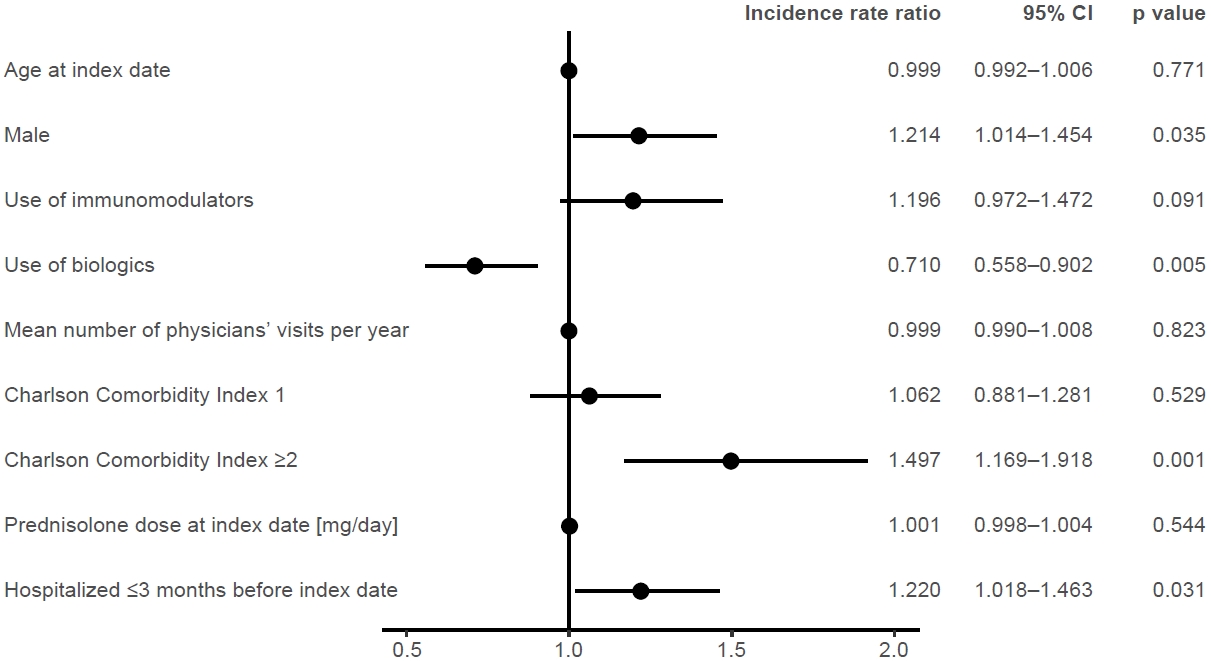
Multivariate regression analyses for association between patient characteristics and prednisolone treatment duration for patients that underwent colonoscopy ≤1 month before or at index date (n=571). CI, confidence interval.
DISCUSSION
This Japanese claims database study explored factors associated with the duration of prednisolone use in patients with UC, with particular attention to the recommended practice of conducting a colonoscopy within 1 month before prednisolone administration. Our findings show that patients who underwent colonoscopy ≤ 1 month before their prednisolone prescription tend to have a shorter duration of steroid use. In addition, shorter durations of prednisolone therapy were associated with higher initial doses at the index date and lower CCI scores at baseline.
Colonoscopy plays a critical role in managing UC for diagnosing the disease, assessing its severity, and monitoring response to treatments [8,9,11,12]. Thus, it is recommended to directly assess the colon whenever a new therapy is started to help optimize treatment [8,12,23]. Of the patients who underwent colonoscopy in our study, most (76%) received it either before, or on the same day, as starting steroids rather than afterwards; this indicates that the technique was being used to diagnose the disease.
Our analysis shows that patients who received colonoscopy within 1 month before starting prednisolone spent less time undergoing the therapy than those who did not receive colonoscopy in this time. These results complement a previous administrative claims database study in the United States, which found that proactive disease monitoring (predominantly through colonoscopy) within 6 months of starting biologics therapy was associated with reduced steroid use and fewer disease-related complications [24]. Therefore, the available evidence supports the steroid-reducing benefits of pretreatment colonoscopy and later endoscopic evaluations for patients with UC. Furthermore, endoscopic healing greatly improves long-term clinical remission, decreases the risk of colectomy, and reduces the need for steroids [8,25]. Patients with UC should thus be regularly assessed to ensure they are meeting disease control criteria [1,18].
Due to the limitations of the source database and retrospective study designs, it is unclear whether the association between short steroid treatment duration and colonoscopy is due to a causative link or a shared correlation with good practice. For instance, studies in the United Kingdom have indicated that steroids are used more appropriately for patients with UC at dedicated inflammatory bowel disease clinics and intervention centers participating in a quality improvement program [26,27]. Similarly, our finding that treatment durations were shorter for patients that received colonoscopy could simply reflect practice that involves both adequate imaging and appropriate steroid management. Regardless, these results imply that colonoscopy around the time of steroid induction may be a useful quality indicator in the management of UC.
The multivariable analysis detected an effect of colonoscopy, whereas the univariate analysis found no association between colonoscopy and the duration of steroid use. This may partly be due to the analytical decision for a 3-month cutoff, but also the effects of other factors including demographics, medications, medical attention, comorbidities, and dose rates, which are not accounted for in univariate analysis. In any case, the importance of other factors alongside colonoscopy in reducing steroid duration is clear. For instance, the sub-analysis on patients who received colonoscopy before steroids suggests an important role of other drugs in reducing steroid duration, as those using biologics spent less time on steroids than those who did not. Overall, colonoscopy is an element of good practice and attendance to the guidelines, and thus any effects it has may only arise when embedded with other recommendations (such as using biologics and prescribing high doses).
The majority of patients in our study received low doses (≤ 30 mg) of prednisolone at induction compared to the standard guideline-recommended dose for UC (30–40 mg/day oral, 40–80 mg/day IV) [1,3]. These results conform to a previous study, also using the JMDC database, which found that 49% to 71% of prednisolone prescriptions were < 30 mg/day during 2010 to 2016 [22]. Furthermore, both this study and ours detected an association between low initial prednisolone doses and longer durations of steroid treatment, possibly because low-dose steroids may be ineffective at suppressing inflammation [22]. Therefore, the results support the use of high initial doses of steroids alongside colonoscopy as elements of good practice.
Explanations for the low initial steroid doses are restricted to speculation due to the inherent limitations of the source database. For instance, individual physicians often bear the responsibility for deciding dose rates on a case-by-case basis and low-dose steroids may have been prescribed according to mild UC severity or the other treatments being provided (i.e., 5-ASA, biologics and/or thiopurine). However, the database does not include information on disease severity or justifications for prescribed dosages to test this hypothesis. Similarly, the result may also be explained if low-dose steroids were prescribed for non-UC diseases, but the database does not indicate the disease for which drugs were prescribed. In our study, however, steroids appear to be prescribed in response to an assessment of UC and not because of other conditions. Specifically, CCI scores were based on comorbidities present during the 3-month look-back period, but steroids were mostly prescribed only after colonoscopy (89.7% of colonoscopies). Furthermore, the distribution of doses for non-comorbid patients indicates that prescriptions for UC alone follow the same trend. Therefore, any further investigation into the low steroid doses among Japanese UC patients awaits research using different methodologies. In any case, the observations of Matsuoka et al. [22] indicate that dose rates have been steadily increasing over time.
Our study showed that patients with comorbidities, as assessed by a CCI score of 1 or ≥ 2, were more likely to have a longer duration of steroid use than those with no comorbidities. Unfortunately, however, the JMDC database does not indicate the disease for which prednisolone (or other drugs) was prescribed when patients had more than one disease code. Therefore, it is unclear whether steroids or other medications were being administered to control non-UC diseases. This is especially relevant if some patients had diagnostic codes with Crohn’s disease or Behçet’s disease in addition to UC. In any case, this finding highlights comorbidities as a factor worthy of further research, given that appropriate steroid use is even more important in patients with comorbidities.
There are several limitations to this study that stem from its retrospective design and source data in addition to those already mentioned. First, steroid use is likely to be closely associated with the extent and severity of the underlying disease, but the database does not provide any information in this regard. Second, we had no information on why steroid treatment was stopped, or whether prolonged use was intentional. Similarly, we had no information concerning treatment adherence, given that we were only able to review prescription data. Third, our study relied on ICD-10 codes for disease diagnosis and thus UC cases were not confirmed by clinical observation. Fourth, the JMDC database does not carry-over records for patients that change insurance, meaning that some records may be incomplete.
Therefore, like any retrospective claims-based database study, our results await confirmation from dedicated experiments and clinical trials. Even so, observational studies such as this play an important role in highlighting factors and patterns deserving further scrutiny, for which our results emphasize colonoscopy, dose rates, and comorbidities. Future research may also benefit by considering calcineurin inhibitors like tacrolimus, which can be used for steroid-dependent or resistant cases.
In conclusion, this study found that performing colonoscopy before or at the time of starting systemic steroid treatment is associated with a shorter duration of steroid use in patients with UC. Our findings may provide useful information for optimal disease management of UC.
Notes
Funding Source
This work was funded by Takeda Pharmaceutical Company Limited.
Conflict of Interest
Kobayashi T has served as a speaker, a consultant, or an advisory board member for AbbVie, Ajinomoto Pharma, Asahi Kasei Medical, Astellas, Alfresa Pharma, Bristol-Myers Squibb, Celltrion, Covidien, EA Pharma, Eisai, Eli Lilly, Ferring Pharmaceuticals, Gilead Sciences, Janssen, JIMRO, Kyorin Pharmaceutical, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, Nippon Kayaku, Pfizer, Takeda Pharmaceutical Company Limited, Thermo Fisher Scientific, and Zeria Pharmaceutical. He has received research funding from AbbVie, Alfresa Pharma, Asahi Kasei Medical, EA Pharma, Kyorin Pharmaceutical, Mochida Pharmaceutical, Nippon Kayaku, Otsuka Holdings, Sekisui Medical, Thermo Fisher Scientific, and Zeria Pharmaceutical. Udagawa E was employed by Takeda Pharmaceutical Company Limited. Hirose L is a current employee of Takeda Pharmaceutical Company Limited. Hibi T has served as a speaker, a consultant, or an advisory board member for AbbVie, AbbVie GK, Aspen Japan K.K, Bristol-Myers Squibb, Celltrion, EA Pharma, Eli Lilly, Ferring, Gilead Sciences, Janssen, JIMRO, Kissei Pharmaceutical, Kyorin, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, Nichi-Iko Pharmaceutical, Nippon Kayaku, Pfizer, Takeda Pharmaceutical Company Limited, and Zeria Pharmaceutical. He has received research funding from AbbVie, EA Pharma, JIMRO, Otuska Holdings, and Zeria Pharmaceutical. And he is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. Except for that, no potential conflict of interest relevant to this article was reported.
Data Availability Statement
This study was conducted using the Japan Medical Data Center database, an employer-based insurance claims database. The database contains monthly claims data submitted to health insurance societies from participating medical institutions and pharmacies since 2005.
Author Contributions
Conceptualization: Kobayashi T, Udagawa E, Hibi T. Data curation: all authors. Methodology: Kobayashi T, Udagawa E. Supervision: Kobayashi T, Hibi T. Writing-original draft: Udagawa E, Hirose L. Writing-review & editing: all authors. Approval of final manuscript: all authors.
Additional Contributions
We thank the Japan Medical Data Center for providing the claims database, Maki Ueyama at Creativ-Ceutical for acquisition of data and statistical analysis. Editorial and writing support was provided by Ngaire White and Stephen Heap at MIMS, and Nicholas Crabb at FireKite, in compliance with international guidelines for Good Publication Practice 3. Statistical and editorial support was funded by Takeda Pharmaceutical Company Limited.