Comparative outcomes of acute colonic diverticulitis in immunocompromised versus immunocompetent patients: a systematic review and meta-analysis
Article information

Abstract
Background/Aims
Immunocompromised patients with acute colonic diverticulitis are at high risk for complications and failure of non-surgical treatment. However, evidence on the comparative outcomes of immunocompromised and immunocompetent patients with diverticulitis is lacking. This systematic review and meta-analysis investigated the outcomes of medical treatment in immunocompromised and immunocompetent patients with diverticulitis.
Methods
A comprehensive literature search was conducted in PubMed, Embase, and the Cochrane Library. Studies comparing the clinical outcomes of immunocompromised and immunocompetent patients with diverticulitis were included.
Results
A total of 10 studies with 1,946,461 subjects were included in the quantitative synthesis. The risk of emergency surgery and postoperative mortality after emergency surgery was significantly higher in immunocompromised patients than in immunocompetent patients with diverticulitis (risk ratio [RR], 1.76; 95% confidence interval [CI], 1.31–2.38 and RR, 3.05; 95% CI, 1.70–5.45, respectively). Overall risk of complications associated with diverticulitis was non-significantly higher in immunocompromised than in immunocompetent patients (RR, 1.24; 95% CI, 0.95–1.63). Overall mortality irrespective of surgery was significantly higher in immunocompromised than in immunocompetent patients with diverticulitis (RR, 3.65; 95% CI, 1.73–7.69). By contrast, postoperative mortality after elective surgery was not significantly different between immunocompromised and immunocompetent patients with diverticulitis. In subgroup analysis, the risk of emergency surgery and recurrence was significantly higher in immunocompromised patients with complicated diverticulitis, whereas no significant difference was shown in mild disease.
Conclusions
Immunocompromised patients with diverticulitis should be given the best medical treatment with multidisciplinary approach because they had increased risks of surgery, postoperative morbidity, and mortality than immunocompetent patients.
INTRODUCTION
Colonic diverticulitis, one of the most common gastrointestinal diseases, is frequently encountered in clinical practice [1]. The incidence of colonic diverticulitis has steadily increased over the past decades, particularly in younger patients [2,3]. Approximately 12% of acute diverticulitis cases manifest as a complicated disease with an abscess, peritonitis, stricture, or fistula [1]. Patients with abdominal sepsis who are hemodynamically unstable require surgical intervention and are at significant risk of mortality [2,4]. Approximately 20% of patients with acute colonic diverticulitis experience at least one recurrence [1]. Several studies have suggested immunosuppression as a risk factor for diverticulitis. Corticosteroid use is associated with an increased risk of complicated diverticulitis [5,6]. Patients with diverticulitis who are immunocompromised may present with milder symptoms and signs than immunocompetent patients but are more likely to present with severe or complicated disease [7]. In addition, immunocompromised patients with diverticulitis are at high risk for failure of non-surgical treatment [7-9]. Therefore, some guidelines recommend antibiotic treatment and early surgical consultation for immunocompromised patients with diverticulitis [10-12].
However, the natural history and clinical outcomes of diverticulitis in immunocompromised patients have yet to be fully elucidated. Most studies of diverticulitis in immunocompromised patients were small and observational, focusing on postoperative outcomes and used heterogenous definitions of immunosuppression. Although a recent systematic review and meta-analysis showed a greater risk of postoperative mortality and morbidity in immunocompromised patients with diverticulitis who underwent operative management [13], evidence on the comparative outcomes of medical treatment in patients with diverticulitis who are immunocompromised is lacking. Therefore, we conducted this systematic review and meta-analysis to compare the clinical outcomes of immunocompromised and immunocompetent patients with diverticulitis.
METHODS
1. Search Strategy
A comprehensive literature search was conducted in PubMed, Embase, and the Cochrane Library from 2000 to August 2022. The search terms included “immunocompromised,” “immunosuppressed,” “immunodeficient,” “colonic,” and “diverticulitis.” Detailed search strategies are presented in Supplementary Material. A manual search of the reference lists of identified studies was conducted to include all relevant articles.
2. Inclusion and Exclusion Criteria
All studies comparing the clinical outcomes of acute colonic diverticulitis between immunocompetent and immunocompromised patients were considered eligible. The inclusion criteria were based on the PICO framework: (1) population, patients with acute diverticulitis; (2) intervention, immunocompromised condition or immunosuppressive treatment; (3) comparator, immunocompetent status; and (4) outcome, need for surgery, complications, mortality, length of hospital stay, and recurrence. The exclusion criteria were as follows: (1) studies that did not include immunocompetent patients as a control; (2) studies that included only patients with surgically diagnosed diverticulitis or in which the diagnostic criteria were vague; (3) studies in which the definitions of immunocompetent and immunocompromised patients were ambiguous; (4) non-original articles including reviews, editorials, opinions, letters, case report, and case series; (5) abstract-only publications; (6) non-human studies; and (7) non-English publications.
3. Study Selection
Two investigators (J.G.L. and S.E.K.) independently screened the literature and selected studies. First, all duplicate articles from multiple databases were removed. Next, irrelevant articles were excluded by inspecting the titles and abstracts. The full texts of the remaining articles were reviewed for eligibility. Any disagreements were resolved by discussion. If consensus could not be reached, a third party (H.J.S.) determined study eligibility. Study selection was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement [14].
4. Data Extraction and Outcome Assessment
Using a standardized collection sheet, data were extracted from the included articles. The characteristics of the studies including the first author, year of publication, study design, study period, number of patients, and study endpoints were examined.
The primary endpoint was the comparison of clinical outcomes including need for surgical intervention (emergency or elective), complications, mortality, length of hospital stay, and recurrence between immunocompromised and immunocompetent patients with acute colonic diverticulitis.
Because this systematic review and meta-analysis did not include individual patients or patient data, ethical approval was not required.
5. Study Quality Assessment
Risk of bias assessment was performed independently by 2 investigators (J.G.L. and S.K.) using the Risk of Bias Assessment Tool for Nonrandomized Studies (RoBANS) version 2.0. RoBANS version 2.0 rates the risk of bias as high, low, or unclear in domains of participant comparability, selection of participants, confounding variables, measurement of exposure, blinding of outcome assessments, outcome evaluation, incomplete outcome data, and elective reporting [15]. Disagreements were discussed among the investigators until consensus was reached.
6. Statistical Analysis
A standard pairwise meta-analysis was conducted to compare clinical outcomes between immunocompromised and immunocompetent patients with acute colonic diverticulitis. Assessment of heterogeneity was performed using Cochrane’s Q test and inconsistency (I2) statistics. We considered I2 > 50% or P < 0.1 to represent significant heterogeneity [16]. In the meta-analysis, a fixed-effect model was used if there was no considerable heterogeneity, and a random-effect model was used if there was considerable heterogeneity among studies. Pooled effect estimates were measured by calculating the risk ratios (RRs) for categorical variables and mean differences for continuous variables with 95% confidence intervals (CIs). Publication bias was not evaluated if the number of included studies was < 10 [17]. Statistical analyses were performed with Review Manager version 5.4 (The Cochrane Collaboration, 2020).
RESULTS
1. Study Selection
A total of 391 potentially relevant articles were identified through a comprehensive literature search. Three other articles were identified by manual searching. In total, 80 duplicate articles were removed and 278 articles were excluded based on the titles and abstracts. Subsequently, 36 full text articles were reviewed for eligibility. Twenty-six articles were excluded because they were abstracts without full text (n = 7), had outdated or inadequate diagnostic definitions (n = 2), were out of scope (n = 1), were review articles (n = 4), were not on PICO (n = 7), were duplicate publications (n = 4), or were in another language (n = 1). Finally, 10 studies were included in the quantitative synthesis. PRISMA flowchart is shown in Fig. 1.
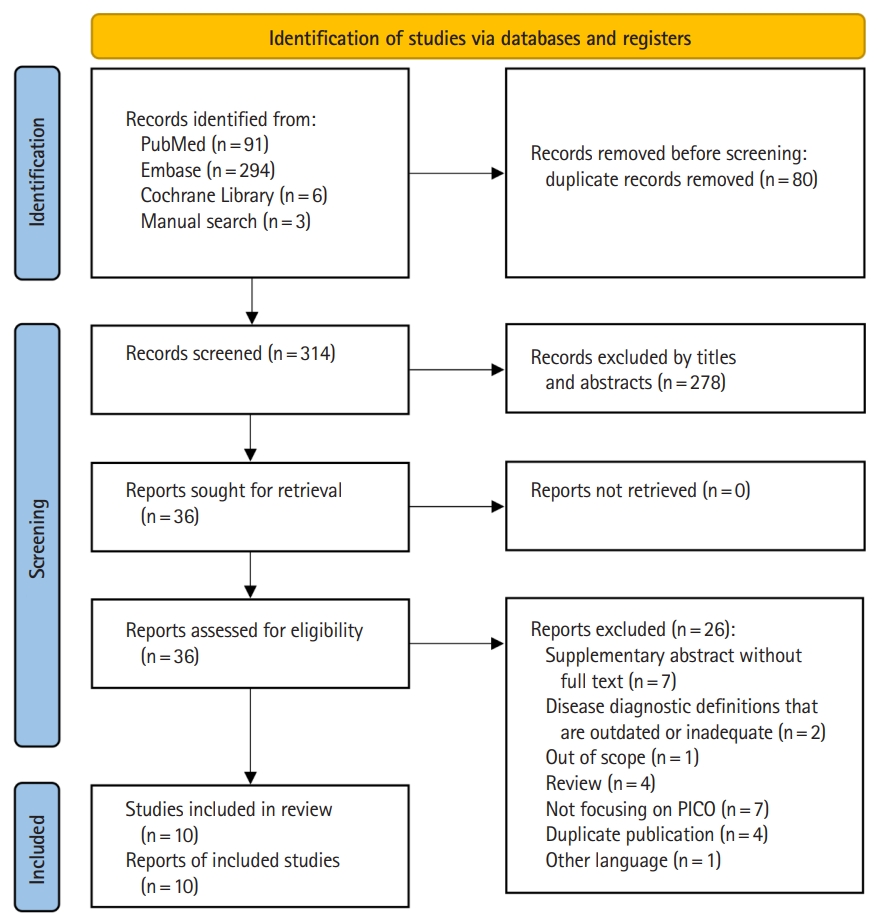
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart.
2. Study Characteristics
Table 1 lists the characteristics of the 10 included studies [7,8,18-25]. Totals of 5,339 immunocompromised patients and 1,941,122 immunocompetent patients with acute diverticulitis requiring hospitalization were analyzed. The study period was 1988 to 2021. All included studies were observational studies. Seven of the 10 studies included patients with sigmoid or left colonic diverticulitis [7,8,18-21,24]. One study included all patients with left or right colonic diverticulitis, but most had sigmoid diverticulitis [22]. The remaining 2 studies did not clarify the location of diverticulitis, but it is presumed that most patients had left colonic diverticulitis considering the contents of their analysis [23,25].

Characteristics of the Included Studies
The definitions of immunocompromised patients were heterogenous, including patients on immunosuppressive agents, chronic corticosteroid treatment, solid organ transplant, nongastrointestinal active malignancy, chemotherapy, collagen vascular disorders, end-stage renal disease, and congenital or acquired immunodeficiency.
3. Risk of Bias
Supplementary Fig. 1 shows the risk of bias assessment. Because all included studies were non-randomized observational studies, we used RoBANS version 2.0 tool to assess the risk of bias. Many studies were rated as unclear in the domains of confounding variables and selection of participants. In the domain of confounding variables, one study was rated as high risk because most immunocompromised patients were likely to have chronic medical illnesses of moderate or greater severity, an unavoidable limitation without statistical adjustment because these can act as confounding variables [8]. In the domain of selection of participants, one study was rated as high risk because the control group might have included patients who were not completely immunocompetent [22].
4. Need for Surgical Intervention
Five of the included studies reported rates of surgical intervention for acute diverticulitis [7,8,19,22,25]. Fig. 2 presents the forest plot of surgery rates. The overall risk of surgical intervention, emergency or elective, was not significantly different between immunocompromised and immunocompetent patients with acute colonic diverticulitis (RR, 1.26; 95% CI, 0.81–1.96). However, the rates of emergency surgery in immunocompromised and immunocompetent patients were 34.3% and 22.4%, respectively, showing a significantly higher risk in the immunocompromised patients (RR, 1.76; 95% CI, 1.31–2.38) in the meta-analysis (Z = 3.71, P = 0.0002, I2 = 37%).
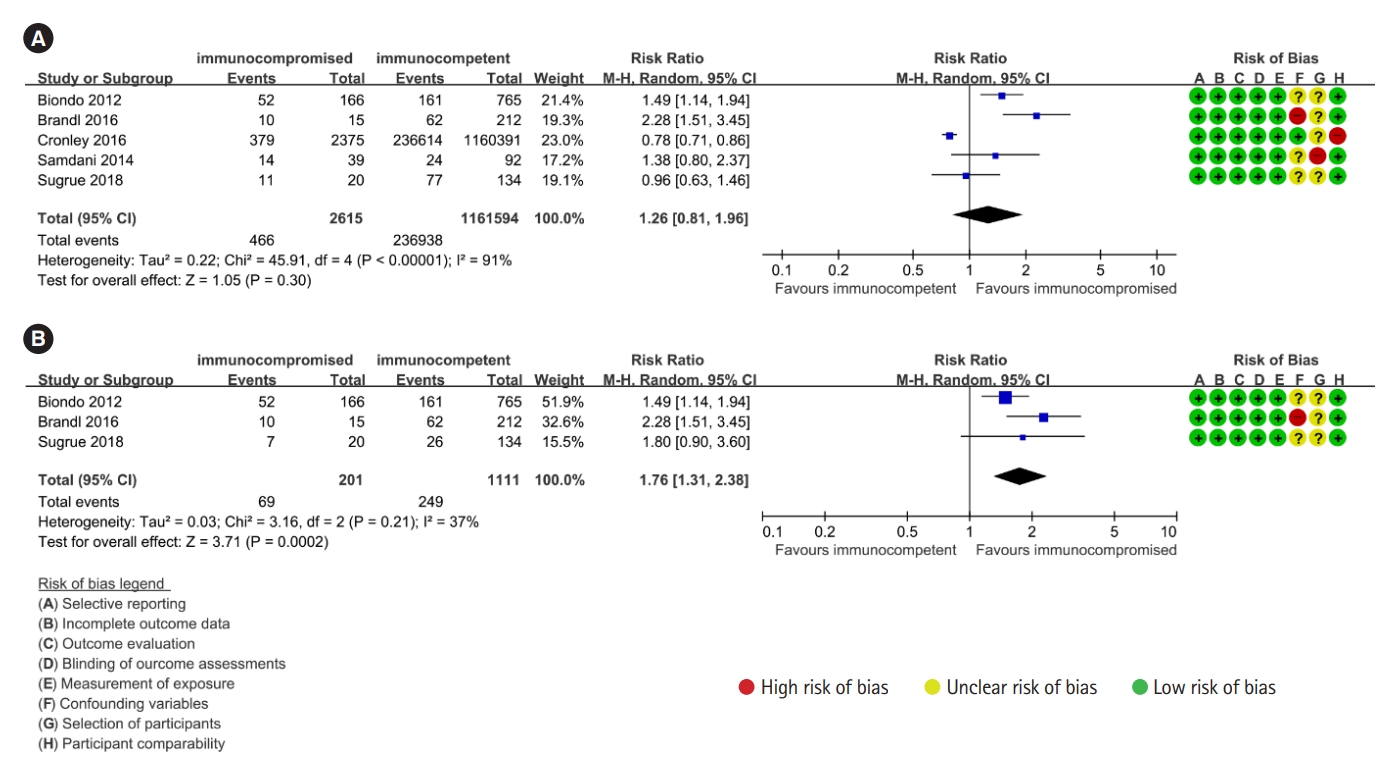
Forest plot of (A) overall need for surgery and (B) emergency surgery in immunocompromised versus immunocompetent patients with acute colonic diverticulitis using a random-effects model. M-H, Mantel-Haenszel; CI, confidence interval.
5. Complications
Four studies reported complications associated with acute diverticulitis [7,8,22,25]. Complications included abscess, perforation, obstruction, or fistula. The overall risk of complications associated with diverticulitis was non-significantly higher in immunocompromised than in immunocompetent patients (RR, 1.24; 95% CI, 0.95–1.63) (Fig. 3).
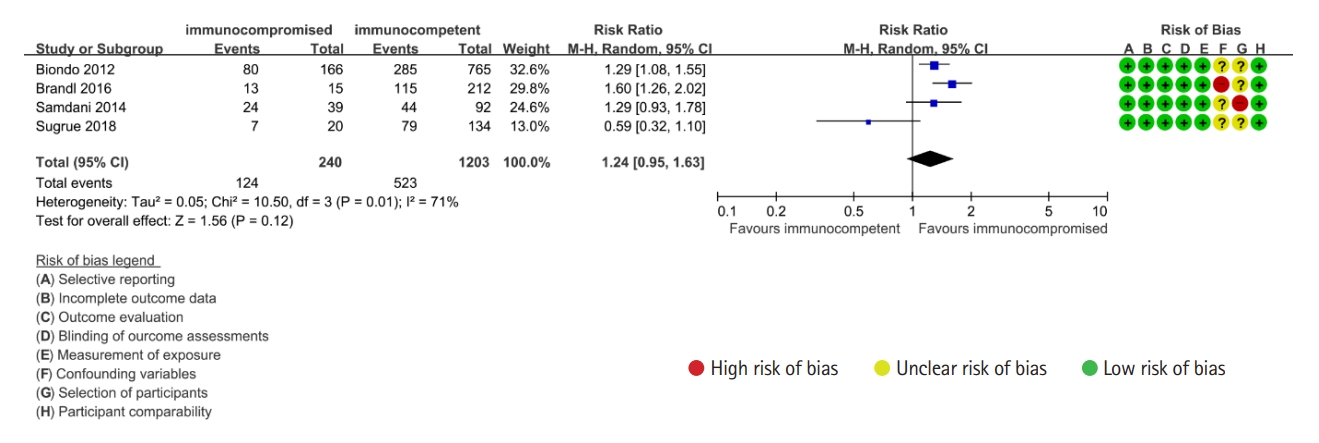
Forest plot of complicated disease of acute colonic diverticulitis in immunocompromised versus immunocompetent patients using a random-effects model. M-H, Mantel-Haenszel; CI, confidence interval.
6. Mortality
Nine of the included studies reported mortality rates [7,8,18-24]. The overall mortality after acute colonic diverticulitis irrespective of surgical intervention was 4.7% in immunocompromised patients and 1.5% in immunocompetent patients. Meta-analysis revealed that the immunocompromised patients had a significantly higher risk of overall mortality (RR, 3.65; 95% CI, 1.73–7.69) (Z = 3.40, P = 0.0007, I2 = 94%). Likewise, in patients who underwent emergency surgery, the risk of death was significantly higher in those with immunosuppression than in those without (RR, 3.05; 95% CI, 1.70–5.45) in the meta-analysis (Z = 3.75, P = 0.0002, I2 = 87%), showing mortality rates of 13.1% and 4.9%, respectively. By contrast, among those who underwent elective surgery, the risk of death was not significantly different between immunocompromised and immunocompetent patients, although the results were significantly heterogeneous (RR, 2.02; 95% CI, 0.03–118.95) in the meta-analysis (Fig. 4).
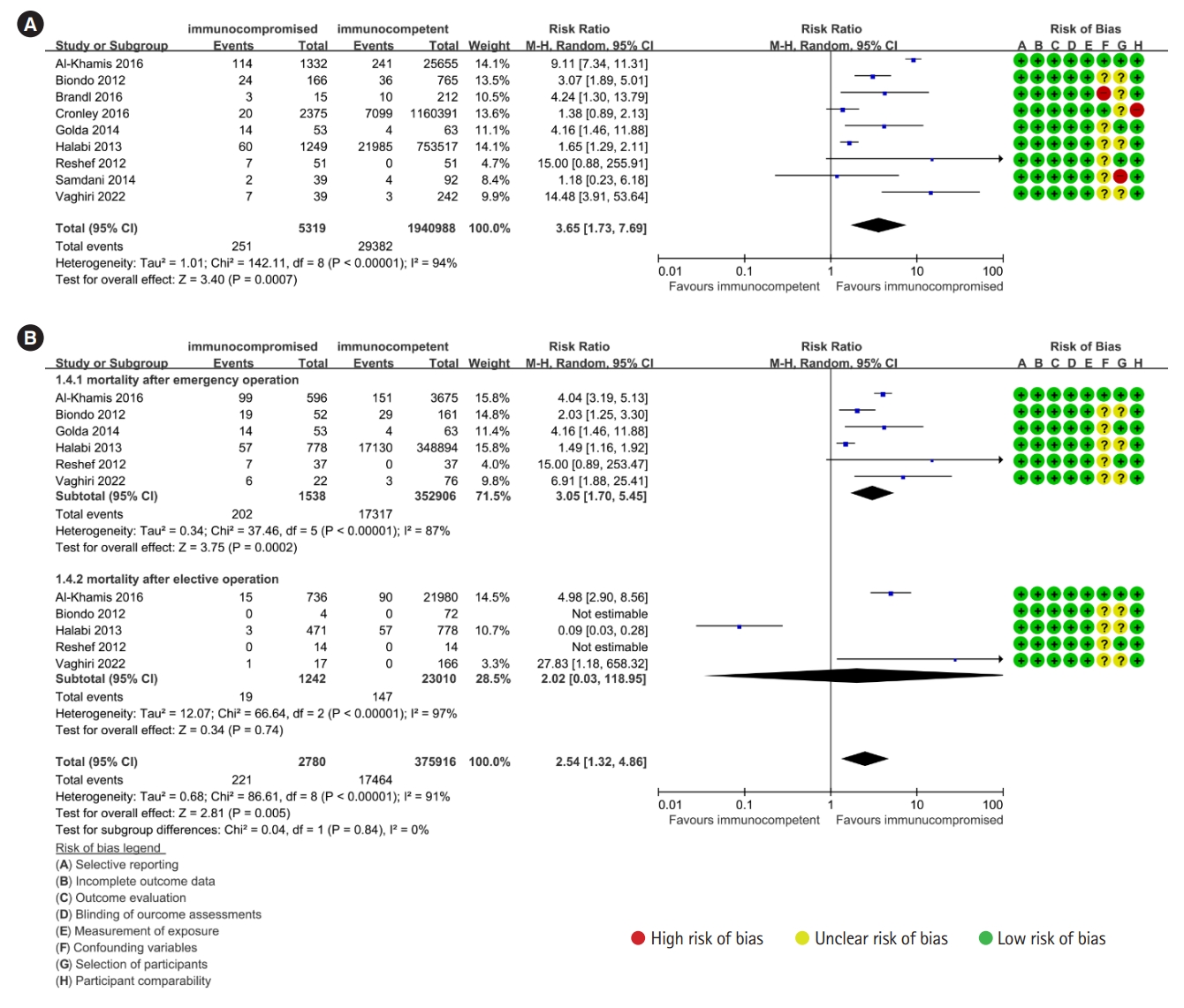
Forest plot of (A) overall mortality and (B) postoperative mortality in immunocompromised versus immunocompetent patients with acute colonic diverticulitis using a random-effects model. M-H, Mantel-Haenszel; CI, confidence interval.
7. Length of Hospital Stay
Six of the included studies reported the length of hospital stay [8,18,20-22]. Fig. 5 shows the forest plot for length of hospital stay. Immunocompromised patients with diverticulitis had a longer hospital stay than immunocompetent patients (mean difference, 6.12; 95% CI, 2.04–10.20).
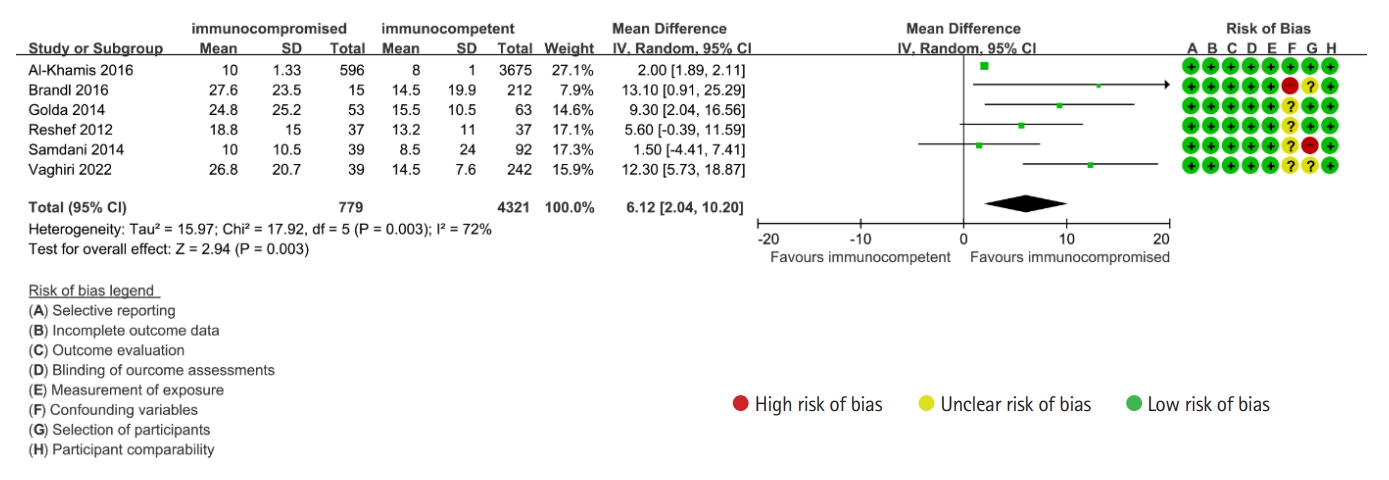
Forest plot of length of hospital stay in immunocompromised versus immunocompetent patients with acute colonic diverticulitis using a random-effects model. SD, standard deviation; CI, confidence interval.
8. Recurrence
Three studies reported recurrence rates after the first episode of diverticulitis [7,22,25]. The duration of follow-up was a median of 33 to 44 months in 2 studies [22,25], and a mean of 81.62 months in 1 study [7]. There was no significant difference in recurrence rates between immunocompromised and immunocompetent patients with acute colonic diverticulitis (RR, 0.96; 95% CI, 0.70–1.33) (Fig. 6).

Forest plot of recurrence rate in immunocompromised versus immunocompetent patients with acute colonic diverticulitis using a fixed-effects model. M-H, Mantel-Haenszel; CI, confidence interval.
9. Postoperative Morbidity after Elective Surgery for Diverticulitis
Four studies reported postoperative morbidities including surgical site infection, wound dehiscence, anastomotic leakage or stenosis, intraabdominal abscess, sepsis, ileus, postoperative bleeding, and cardiovascular, pulmonary, thromboembolic, and renal and urinary tract complications [18,21,22,24]. The rates of postoperative morbidities after elective colonic resection in immunocompromised and immunocompetent patients were 26.6% and 12.3%, respectively. Immunocompromised patients with diverticulitis had a greater risk of postoperative morbidity than immunocompetent patients (RR, 2.07; 95% CI, 1.83–2.34) in the meta-analysis (Z = 11.58, P < 0.00001, I2 = 45%) (Fig. 7).
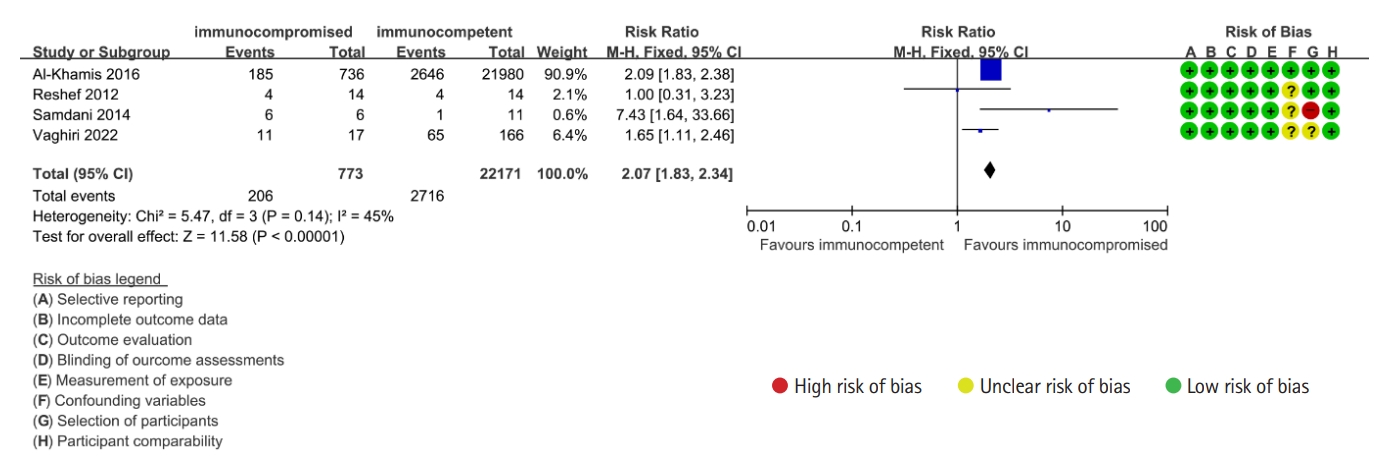
Forest plot of major morbidity after elective surgery for acute colonic diverticulitis in immunocompromised versus immunocompetent patients using a fixed-effects model. M-H, Mantel-Haenszel; CI, confidence interval.
10. Subgroup Analysis by Disease Severity
To examine the clinical outcomes according to disease severity, subgroup analyses were performed. Two studies reported clinical outcomes according to disease severity [7,25]. Severe disease was defined as complicated diverticulitis with an abscess or perforation, and mild disease as diverticulitis without an abscess or perforation.
The risk of emergency surgery following the failure of medical treatment was not significantly different between immunocompromised and immunocompetent patients with mild diverticulitis (RR, 1.13; 95% CI, 0.51–2.50). On the contrary, immunocompromised patients with severe diverticulitis had a greater risk of emergency surgery following failure of medical treatment as compared with their immunocompetent counterparts (55.2% vs. 39.3%; RR, 1.77; 95% CI, 1.10–2.84) (Supplementary Fig. 2).
The risk of recurrence was significantly lower in immunocompromised patients with mild diverticulitis than in immunocompetent patients (RR, 0.50; 95% CI, 0.27–0.91). However, immunocompromised patients with severe diverticulitis showed a greater risk of recurrence as compared with immunocompetent patients (RR, 3.67; 95% CI, 1.58–8.50) (Supplementary Fig. 3).
There was a limitation of this subgroup analysis in that neither study was large. Moreover, the proportion of immunocompromised patients who underwent elective surgery after mild diverticulitis was not clarified in one study [7], which may have affected the recurrence rate.
DISCUSSION
In this systematic review and meta-analysis, immunocompromised patients with diverticulitis had significantly increased risks of surgical intervention, postoperative morbidity, and mortality than immunocompetent patients. Also, the length of hospital stay was longer in immunocompromised than in immunocompetent patients.
Our results support current recommendations that immunocompromised patients with diverticulitis should be treated rigorously. Although recent evidence suggests that antibiotic treatment has no significant benefit in immunocompetent patients with uncomplicated diverticulitis [26,27], it is still recommended for patients with immunosuppression even if there are no complications [10-12]. Additionally, current guidelines recommend that surgeons should maintain a low threshold for surgical intervention in immunocompromised patients with diverticulitis because medical treatment is more likely to fail in such persons [28]. Our results demonstrated that immunocompromised patients had an approximately 1.8-fold increased risk of emergency surgery and a 3.7-fold increased overall risk of death compared with their immunocompetent counterparts. The risk of postoperative mortality after emergency surgery was significantly higher in immunocompromised patients, whereas the risk of postoperative mortality after elective surgery was not significantly different between immunocompromised and immunocompetent patients with diverticulitis. In addition, the risk of complications associated with diverticulitis also tended to increase in immunocompromised patients with diverticulitis, although it was not statistically significant. Furthermore, immunocompromised patients with complicated or severe diverticulitis had increased risks of emergency surgery and recurrence. In one study, when recurrence occurred in patients who had had severe or complicated diverticulitis, severe or complicated disease was repeatedly seen in > 70% irrespective of immune status, and > 20% of these recurrent patients underwent emergency surgery [7]. Therefore, acute diverticulitis in patients with immunosuppression should be recognized as a medical emergency requiring immediate medical attention and multidisciplinary management. Because immunocompromised patients are vulnerable to invasive treatments and have a high risk of death after emergency surgery, they should be given the best nonoperative management unless emergency surgery is unavoidable. Early identification of immunocompromised patients as a high-risk group, prompt evaluation, and early initiation and step-up of antibiotic treatment are required. Meanwhile, in case of complicated or severe diverticulitis, elective surgical intervention can be considered if the patient is medically fit for surgery, because complicated diverticulitis in immunocompromised patients is likely to recur repeatedly as a complicated disease.
However, further discussion is needed on whether aggressive treatment including surgery is essential for immunocompromised patients with mild uncomplicated diverticulitis. Previous studies have shown that there was no significant difference in the outcomes of nonoperative management between immunocompromised and immunocompetent patients with mild uncomplicated diverticulitis [7,25]. Our results also demonstrated that the risk of emergency surgery following failure of medical treatment and the risk of recurrence in mild uncomplicated diverticulitis were not significantly different between immunocompromised and immunocompetent patients, although the results were not robust. Another potential reason why elective surgery is considered unlikely to be necessary in immunocompromised patients with mild uncomplicated diverticulitis is that the overall risk of major morbidity after elective surgery for diverticulitis in immunocompromised patients is more than 2-fold that in immunocompetent patients. Because most included studies did not present treatment outcomes according to disease severity, definite conclusions cannot be drawn from our results. We suggest that immunocompromised patients with mild uncomplicated diverticulitis should receive the best medical treatment and be closely monitored for complications.
There is insufficient evidence on whether immunocompromised patients with diverticulitis are more likely to develop recurrent disease. Our results showed that there was no significant difference in recurrence rates between immunocompromised and immunocompetent patients, although the results were not robust due to the small number of included studies. However, in a subgroup analysis according to disease severity, immunocompromised patients with complicated diverticulitis had a greater risk of recurrence. Current guidelines suggest that patients with immunosuppression should consult a surgeon to discuss elective surgical resection after recovery from an acute episode of diverticulitis especially in complicated cases [12,29,30]. This recommendation seems reasonable because immunocompromised patients are more likely to present with complicated recurrent disease [7,22]. However, it is unclear whether elective surgical resection increases overall survival in immunocompromised patients because they are likely to be frail and have a high risk of postoperative complications [31]. Our results also indicated that immunocompromised patients with diverticulitis had a greater risk of postoperative morbidity after elective surgery than immunocompetent patients. Further research is needed on the long-term survival of immunocompromised patients with diverticulitis who undergo elective surgical resection. The serious clinical impact of recurrence on immunocompromised patients who have not undergone elective surgery after colonic diverticulitis must be carefully considered on a case-by-case basis.
The mechanisms of increased risk of life-threatening diverticulitis in immunocompromised patients are unclear. Plausible explanations include impaired healing leading to bowel perforation, and a lack of immune response that masks symptoms [1]. Immunosuppressive agents have been suggested to impair wound healing and increase the increased risk of wound complications [32,33]. Colonic diverticulitis is thought to arise from complex interactions among diet, lifestyle, genetic factors, and an altered gut microbiome [1]. The pathophysiology of diverticulitis in the immunocompromised settings is uncertain, warranting further research to delineate the mechanisms of developing complicated diverticulitis in immunocompromised patients.
Caution is needed when applying the results of this study to patients with right colonic diverticulitis. Most diverticulitis occurs in the left colon in Western countries. By contrast, most diverticulitis occurs in the right colon in Asia, although the incidence of left-sided diverticulitis has increased in recent years. Previous studies have shown that approximately 80% of colonic diverticulitis is located in the right colon in East Asia [34,35]. Right colonic diverticulitis has a lower risk of complications requiring surgical intervention and a relatively good prognosis than left colonic diverticulitis [36]. Because almost all studies included in this meta-analysis investigated the outcomes of left colonic diverticulitis, the severity and prognosis of right colonic diverticulitis in immunocompromised patients cannot be determined. More data are needed to determine the natural course and prognosis of right colonic diverticulitis in the immunocompromised.
The results of this study can be valuable evidence for medical treatment strategies for immunocompromised patients with diverticulitis. Although a systematic review and meta-analysis on the clinical outcomes of immunocompromised patients with diverticulitis was recently conducted, it assessed the postoperative outcomes in patients who underwent surgical intervention [13]. We quantified not only postoperative outcomes but also overall complication rates, mortality, length of hospital stay, and recurrences in immunocompromised patients with diverticulitis. In addition, we excluded old studies that involved patients with only surgically diagnosed diverticulitis without radiologic examinations, which were likely to have a selection bias of not recruiting patients with mild diverticulitis that did not require surgery or with unknown disease severity [9,37].
This study has several limitations. All included studies were observational, and most were retrospective. Second, the definitions of immunocompromised patients were heterogeneous; patients on immunosuppressive drugs, organ transplant recipients, and those with active extracolonic malignancies, chemotherapy, collagen vascular disease, pulmonary fibrosis, emphysema, end-stage renal disease, and congenital or acquired immunodeficiency syndrome were classified as immunocompromised. Old age itself can be an immunocompromised condition, but it was not considered in the analysis. Because there is no universally accepted definition of immunocompromised patients, there may be inherent flaws in the literature search. Additionally, the difference in clinical outcomes according to the cause of immunosuppression could not be determined. Third, almost all included studies examined the outcomes of left colonic diverticulitis.
Despite these limitations, our findings provide insight into the clinical outcomes of acute colonic diverticulitis in immunocompromised patients. Immunocompromised patients with diverticulitis have greater risks of surgical intervention, postoperative morbidity, and mortality than their immunocompetent counterparts. Early identification, timely evaluation, and the best medical treatment with multidisciplinary approach should be given to immunocompromised patients with acute colonic diverticulitis.
Notes
Funding Source
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
Park YE, Chang JY, and Kim DK are editorial board members of the journal but were not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Data Availability Statement
Not applicable.
Author Contribution
Conceptualization: Kim SE. Data curation: Kim SE, Lee JG. Formal analysis: Kim SE, Lee JG. Methodology: Park YE, Chang JY, Song HJ, Kim DH, Yang YJ, Kim BC, Lee SH, You MW. Supervision: Kim SE. Writing - original draft: Lee JG. Writing - review & editing: Kim SE, Lee JG. Approval of final manuscript: all authors.
Supplementary Material
Supplementary materials are available at the Intestinal Research website (https://www.irjournal.org).
Supplementary Material. Detailed Search Strategy
ir-2023-00005-Supplementary-1.pdfSupplementary Fig. 1. Risk of bias assessment of included studies.
ir-2023-00005-Supplementary-Fig-1.pdfSupplementary Fig. 2. Forest plot of emergency surgery following failure of medical treatment according to the disease severity in immunocompromised versus immunocompetent patients with diverticulitis using a fixed-effects model. M-H, Mantel-Haenszel; CI, confidence interval.
ir-2023-00005-Supplementary-Fig-2.pdfSupplementary Fig. 3. Forest plot of recurrence rate according to the disease severity in immunocompromised versus immunocompetent patients with diverticulitis using a fixed-effects model. M-H, Mantel-Haenszel; CI, confidence interval.
ir-2023-00005-Supplementary-Fig-3.pdf