Serrated neoplasia pathway as an alternative route of colorectal cancer carcinogenesis
Article information
Abstract
In the past two decades, besides conventional adenoma pathway, a subset of colonic lesions, including hyperplastic polyps, sessile serrated adenoma/polyps, and traditional serrated adenomas have been suggested as precancerous lesions via the alternative serrated neoplasia pathway. Major molecular alterations of sessile serrated neoplasia include BRAF mutation, high CpG island methylator phenotype, and escape of cellular senescence and progression via methylation of tumor suppressor genes or mismatch repair genes. With increasing information of the morphologic and molecular features of serrated lesions, one major challenge is how to reflect this knowledge in clinical practice, such as pathologic and endoscopic diagnosis, and guidelines for treatment and surveillance.
INTRODUCTION
Colorectal cancer (CRC) holds the third rank in cancer incidence and the major cause of cancer-related death in the world.1 In Asia, the incidence of CRC rapidly increased between 1998 and 2007, and CRC became the leading cause of cancer-related death.2
For two decades, conventional adenomas were considered the only precancerous lesions of CRC.3 However, other type of colonic lesions have been considered to have malignant potential which progress via the alternative serrated neoplasia pathway.456789 Circumstantial evidence has shown that the serrated neoplasia pathway contributes to the development of 15% to 30% of all CRCs.41011 The latest World Health Organization (WHO) guideline published in 2010 described sporadic serrated polyp lesions have a typical serrated (“saw-tooth” or stellate) architecture of the crypt lining epithelium. Sporadic serrated polyps are subdivided into sessile serrated adenoma/polyps (SSA/Ps), traditional serrated adenomas (TSAs), and hyperplastic polyps (HPs).12
Clinically, a large portion of post-colonoscopy interval cancers are suspected of developing from serrated polyps.13141516 The development of high resolution endoscopic equipment and an improvement of colonoscopy quality has enhanced recognition of serrated lesions, such as right-sided flat lesions with indiscrete margins.17
The purpose of this review is an overview of the clinicopathological and molecular features of alternative serrated pathway in colorectal carcinogenesis to promote better management and clinical outcomes.
CLASSIFICATION OF SERRATED PRECURSORS
1. Hyperplastic Polyps
HPs are the most prevalent (60%–75%) serrated lesions.1819 Twenty-five percent of the average risk individuals have 1 or more HPs, which are located in left side colon.18 HPs are generally equal to or smaller than 5 mm with a flat or sessile endoscopic feature.20 Histopathologic characteristics of HPs include elongated crypts with proliferation and serration of the upper crypts without cytological atypia.21
HPs can be subclassified on the basis of mucin type into microvesicular HPs (MVHPs), goblet-cell-rich HPs (GCHPs), and mucin-poor HPs (MPHPs).12 MVHP is the most common subtype, accounting for 60% of HPs.20 Histologically, MVHPs are characterized by columnar cells with lots of microvesicular mucin and stellate crypt openings.722
Because MVHPs commonly exhibit BRAF mutations (80%) and occasionally present increased CpG island methylation, 2324 especially in proximal lesions, they are considered precursors of SSA/Ps. When they are large and located in the right colon, it is difficult to distinguish MVHPs from SSA/Ps.
GCHPs account for 30% of HPs252627 and have more rounded crypt openings than MVHPs, showing abundant mature goblet cells in the upper crypt with tendency of left-sided location in colon.2228 GCHPs are linked to KRAS mutations which are presented in approximately 50% of cases,2429 suggesting the possibility of progression to TSAs.30 MPHPs, the rarest form of HPs, lack goblet cells, and are considered a variant of MVHPs developed from reactive change with unknown clinical significance.31
2. Sessile Serrated Adenomas or Polyps
SSA/Ps are comprised of 20% to 35% of colorectal serrated lesions.1819 SSA/Ps were first mentioned by Torlakovic et al.2232 in 1996, but before 2003, SSA/Ps were labeled HPs.6 Current SSA/Ps were defined by WHO classification.12 However, the terminology has remained controversial. Recently, the British Society of Gastroenterology suggested that it should be renamed to “sessile serrated lesions” because it shows neither cytologic dysplasia nor polypoid morphology.3334
The diagnosis of SSA/Ps has increased as our knowledge of this entity grows, both endoscopically and pathologically. 203536 However, the prevalence of SSA/Ps is thought to be underestimated, because there was some discrepancy between expected SSA/P detection rate and actual detection rate of 16% and 12%, respectively in patients with an average CRC risk.1837 In addition, SSA/Ps are most commonly located proximally, but 20% to 40% are also detected in the distal colon.1838
SSA/Ps are histopathologically characterized by patterns including irregular branching, dilation towards the base, and L-shaped or inverted T-shaped crypts (Fig. 1). The inverted crypts can be found below the muscularis mucosa, which is designated as displaced crypts or pseudoinvasion.1221 In addition, SSA/Ps can have cytologic dysplasia, which is more progressive form in adenoma carcinoma sequence.12 Previous studies reported the prevalence of SSA/Ps with dysplasia as 20% to 30% of entire SSA/Ps.1838 The median age of patients with SSA/Ps without dysplasia was 61 years, which with SSA/Ps with dysplasia was 66 years, and which with SSA/P with early cancer was 72 years. This increasing tendency of median age of prevalence indicates their serial progression.9 Meanwhile, the differentiation of SSA/P from MVHP is difficult, especially in small lesions.39 Therefore, a recent consensus recommended that a single characteristic crypt base is enough to diagnose SSA/P, and MVHPs larger than 10 mm should be considered equivalent to SSA/Ps for clinical or surveillance purposes.20

Endoscopic and histologic features of sessile serrated polyps and traditional serrated adenoma. Endoscopic appearance of sessile serrated adenoma (SSA) with white light endoscopy shows smooth and indistinct surface pattern covered with mucus (A). Chromoendoscopy after indigo carmine dye spraying in SSA shows clear boundaries and characteristic pit pattern (type II-O) (B, C). Microscopic features of SSA show irregular branching and T-shaped or L-shaped basal crypt (H&E, ×400) (D). Endoscopic appearance of traditional serrated adenoma (TSA) shows protruded polypoid shape with villous surface (E), and microscopic feature of TSA shows villous serration with dysplasia (H&E, ×40) (F).
3. Traditional Serrated Adenomas
TSAs, the rarest subtype of serrated lesions,181929 are usually pedunculated in shape, and located in the left colon and rectum (Fig. 1).204041 Histologic differentiation of TSAs from tubulovillous adenomas is more difficult than histologic differentiation of SSA/Ps.1221 TSAs are serrated and show villous or tubulovillous configuration that is composed of columnar cells with intensively and diffusely eosinophilic cytoplasm (Fig. 1).202142 Ectopic crypt foci is another important finding of TSAs, which are small aberrant crypts that develop horizontally without anchoring to the underlying muscularis mucosa.21 Cytologic dysplasia (90% low-grade and 10% high-grade) is also commonly presented in TSAs.1221
Filiform serrated adenoma is a rare, less aggressive variant form of TSAs that is characterized by thin and elongated projection lined by neoplastic epithelium.4344
SERRATED NEOPLASIA PATHWAY
Three molecular pathways of CRC carcinogenesis have been established: (1) chromosomal instability (CIN); (2) microsatellite instability (MSI); and (3) CpG island methylator phenotype (CIMP), which is also referred to the serrated neoplasia pathway or epigenetic instability pathway. These pathways are related with each other in complex way in carcinogenesis, and the serrated neoplasia pathway is considered to be separated from traditional pathway (Fig. 2).42645
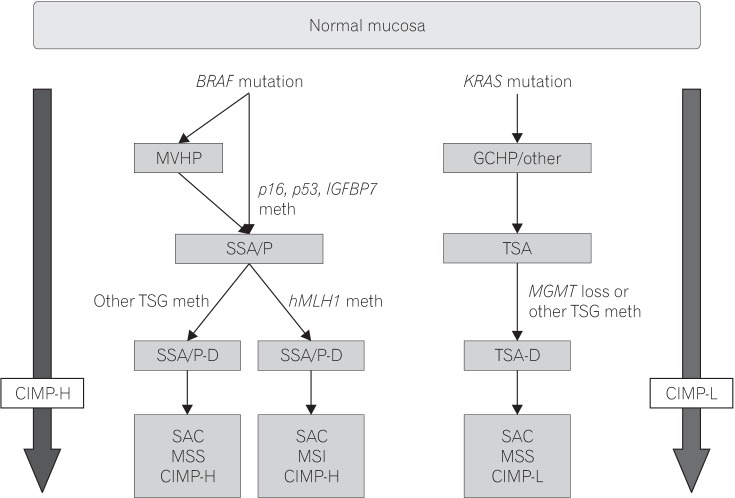
Simplified models of the sessile and traditional serrated pathways. MVHP, microvesicular hyperplastic polyp; GCHP, goblet cell-rich hyperplastic polyp; IGFBT7, insulin-like growth factor-binding protein 7; SSA/P, sessile serrated adenoma/polyp; TSA, traditional serrated adenoma; TSG, tumor suppressor gene; hMLH1, human MutL homolog 1; MGMT, O-6-methylguanine-DNA methyltransferase; SSA/P-D, SSA/polyp with dysplasia; TSA-D, TSA with dysplasia; SAC, serrated adenocarcinoma; meth, methylation; MSS, microsatellite stable; CIMP-H, CpG island methylator phenotype-high; MSI, microsatellite instability; CIMP-L, CpG island methylator phenotype-low.
Hypermethylation of CpG islands on the promoter regions of tumor suppressor genes and subsequent silencing is common in CRC. For example, silencing of hMLH1 leads to mismatch repair (MMR) dysfunction, which results in sporadic MSI. This CIMP, was observed in 20% to 30% of CRC and is one of the major molecular characteristics of the serrated neoplasia pathway.4647 In a previous study, CIMP was detected in 11% of MVHPs and 40% of SSA/Ps.48 CIMP was found not only in serrated polyps, but also in histologically normal mucosa of patients with hyperplastic polyposis syndrome, which supports that CIMP is an important early step of the serrated pathway.495051 In addition, hypermethylation of hMLH1 gene, a DNA MMR gene, was detected in 40% of sporadic CIMP+ CRC. When it is inactivated by hypermethylation, high frequency MSI (MSI-high) is induced, and these lesions tend to develop additional mutations, including BAX, PTEN, MSH3, MSH6, and IGF2R.52 As a result of these mutations, rapid development of cytologic dysplasia and carcinomatous transformation may occur. Relatively rapid development of CRC by the serrated pathway is suggested in the literature, comparable with carcinogenesis in patients with Lynch syndrome.53 In addition, Bettington et al.54 reported 74.5% loss of hMLH1 in SSA/Ps containing dysplasia/carcinoma, showing its relationship with older age, female gender, proximal location, CIMP, and lack of aberrant p53.
Prior to CIMP, a mutation in the BRAF proto-oncogene is the most pronounced key feature in the initial phase of the serrated neoplastic pathway (MSI high and/or CIMP high CRC), which activates the mitogen activated protein kinase (MAPK) cascade. This BRAF mutation results in uncontrolled cell proliferation, similar to KRAS mutation in adenomas. Incidence of BRAF mutation has been reported as 50% to 72% of MVHPs, 70% to 80% of SSA/Ps, and only 1% of tubular adenomas.2555 Because of the exclusive mutation between BRAF and KRAS, however, KRAS mutations were reported to have low prevalence in CIMP-high CRCs.56
Mutations of BRAF or KRAS activate cell proliferation, which is followed by cell senescence.57 If tumor suppressor genes are silenced, as with methylation of p16INK4a or p53 mutations, BRAF or KRAS-induced senescence can be avoided with progression of carcinogenesis.585960 Silencing by methylation of insulin-like growth factor binding protein 7 (IGFBP7), an important mediator of p53 induced senescence, also induces an escape from cell senescence.61
Furthermore, the Wnt signaling pathway, a major signaling pathway of CIN+ CRC, could be involved in the serrated neoplastic pathway. For example, some reports showed that aberrant β-catenin accumulation was detected in 0 out of 19 HPs and 9 out of 22 (41%) SSA/Ps.62 Another study reported aberrant β-catenin accumulation in 8 out of 27 (29%) SSA/Ps without dysplasia and 27 out of 27 (100%) SSA/Ps with dysplasia, suggesting that the Wnt pathway is involved in progression of SSA/Ps, rather than early change of SSA/Ps.56 The mechanism and role of the Wnt signaling in the serrated pathway is not well understood, but silencing by methylation of mutated in colorectal cancer gene (MMC), which correlates with BRAF mutation and CIMP, might have an important role because MMC suppress Wnt signaling via interactions with β-catenin.24
The molecular pathway of TSA development is not well understood. However, it is characterized by promoter hypermethylation and subsequent silencing of the methylguanine methyltransferase (MGMT), KRAS mutation, and CIMP low tumor.426364
ENDOSCOPIC DIAGNOSIS AND MANAGEMENT
Clinically, serrated polyps are considered to be related with the development of interval CRCs. Therefore, endoscopic detection and complete removal is important.65 Endoscopic detection rates of SSA/Ps vary because these lesions are frequently flat and resemble folds of the proximal colon. Magnifying chromoendoscopy and narrow-band imaging (NBI) can facilitate distinction of serrated lesions, but it is not enough to differentiate between SSA/Ps and HPs.66
For detection and diagnosis, it is important to know the distinct features of SSA/Ps (Fig. 1). HPs are usually smaller than 5 mm, and have a pale color and a stellate type II Kudo pit pattern on chromoendoscopy or NBI.6768 The endoscopic features of SSA/Ps are sessile or flat morphology, pale color, indistinct borders with mucus capping, and rim of bubbles or debris.69707172 With NBI, a cloud-like surface, dark spots inside crypts, and type II-O or open Kudo pit pattern, which is wider and more rounded than type II pit pattern, are highly predictive of SSA/Ps.72 Meanwhile, TSAs show protuberant and/or pedunculated shape with a type IV pit pattern and a fern-like feature.7374 In addition, HPs and TSAs tend to locate in the distal part of colon, while SSA/Ps are more frequently observed in the proximal colon.9192975
There is no conclusive evidence-based guideline on management of serrated polyps, but new guidelines recommend that all serrated polyps should be endoscopically removed, except small and diminutive HPs in the rectosigmoid area. SSA/Ps are reported to have higher incomplete resection rates due to their flat shape and indiscrete borders.76 Chromoendoscopy contrast dye can be used to define the border of these lesions,630 and lifting of the lesion is helpful in identifying accurate margins. Therefore endoscopic mucosal resection is an appropriate method for endoscopic teatment.6 If the lesion is not suitable for endoscopic resection due to difficult location or huge size, segmental colectomy is advised.77
As for surveillance after removal of serrated polyp, U.S. Multi-Society Task Force recommended 5-year surveillance interval for SSA/Ps smaller than 10 mm without dysplasia,78 which is shorter than 10 years recommended by European Society of Gastrointestinal Endoscopy guideline.79 Most guidelines recommended 3-year interval for SSA/Ps equal or larger than 10 mm, SSA/Ps with dysplasia, and TSAs.787980 After piecemeal resection of large SSA/Ps, follow-up within 6 months is recommended, consistently.
CONCLUSIONS
In the past two decades, as our knowledge of the morphologic and molecular features and clinical meaning of serrated lesions increased, its detection and diagnosis rate has been improved. Now, we should consider about how to reflect this knowledge in clinical practice, such as pathologic and endoscopic diagnosis, and guidelines for treatment and surveillance. Further investigations about the molecular mechanisms, natural history, and management strategies are needed.
Notes
FINANCIAL SUPPORT: The authors received no financial support for the research, authorship, and/or publication of this article.
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION: Conceptualization, writing - review and editing, approval of final manuscript: Tae Il Kim. Writing - original draft: Soon Young Kim.