Exclusive enteral nutrition for induction of remission in anti-tumor necrosis factor refractory adult Crohn’s disease: the Indian experience
Article information

Abstract
Background/Aims
Exclusive enteral nutrition (EEN) is recommended for induction of remission in pediatric Crohn’s disease (CD). However, it is not currently recommended for inducing remission in adults. This report describes the use of 12-week EEN for induction of remission in anti-tumor necrosis factor (anti-TNF) refractory adult CD.
Methods
This is a retrospective analysis of adults with moderate to severe active (Crohn’s Disease Activity Index [CDAI] >220) anti-TNF refractory CD, who received EEN for 12 weeks between April 2018 and March 2019 at Dayanand Medical College and Hospital, Ludhiana, India. Primary outcomes included achievement of clinical remission and fistula healing at 12 weeks. Improvement in inflammatory markers and nutritional status were the secondary end points.
Results
Out of 23 patients who received anti-TNF agents, 7 (30.4%) were refractory and were offered EEN as a salvage therapy. Six patients (66.7% females, mean age 25.6±6.5 years) consented. Four patients (66.6%) achieved clinical remission (CDAI <150). Mean CDAI of patients decreased significantly after 12 weeks of EEN (388.8±74.8 vs. 160.0±25.2, P<0.001). Perianal fistulas showed clinical response (drainage decreased by >50%), though none achieved remission. Entero-enteric fistulae showed complete healing. Mean body mass index improved from 15.6±3.1 to 18.9±1.9 kg/m2 at week 12 (P=0.003). Hemoglobin and serum albumin also improved from 8.2±1.1 g/dL and 2.8±0.3 g/dL at baseline to 12.6±0.6 g/dL and 3.6±0.5 g/dL post-EEN respectively (P<0.001 and P=0.006 respectively).
Conclusions
EEN appears to be an effective and well tolerated therapy for induction of remission in anti-TNF refractory adult CD. More data from prospective trials with larger number of patients is required.
INTRODUCTION
Crohn’s disease (CD) is a chronic and progressive transmural inflammatory disease of the digestive tract characterized by a relapsing-remitting clinical course. Therapeutic options for active CD include corticosteroids, immunomodulators and biologics including anti-TNF agents [1]. However, about one-third of patients are primary nonresponders to anti-TNF agents and another one-third are secondary nonresponders [2-5]. Therapeutic options in these patients are limited to newer biologics like vedolizumab (anti-integrin) and ustekinumab (antagonizes interleukin 12 and interleukin 23 through their common p40 subunit) [6], leucocytapheresis [7], granulocyte and monocyte adsorptive apheresis [8], or surgery. However, data concerning their efficacy for inducing remission are scant and conflicting [6,8,9]. The spectrum of therapeutic arsenal is further narrowed in patients with complicated (fistulizing/stricturing) disease as majority of these patients are unfit for surgical interventions in view of poor nutritional status [10,11].
Historically, supplementation of nutrition has been an adjunctive therapy for management of IBD. More recently however, nutrition has been evaluated as a primary therapeutic option for management of IBD in the form of exclusive or partial enteral nutrition [12]. Exclusive enteral nutrition (EEN) involves the use of a complete liquid diet, with exclusion of normal dietary components for a defined period of time, as a therapeutic measure and has an accepted role in induction of remission in active pediatric CD [13-15]. EEN however is not recommended currently for induction of remission in adults as it has not been found superior to corticosteroids and other pharmacological agents. Most of the initial studies evaluating the efficacy of EEN in adult CD excluded patients with stricturing/fistulizing disease [16-18]. However, recent cohort studies in steroid nonresponsive patients have provided evidence for efficacy of EEN for induction as well as maintenance of remission in adults with complicated CD [19-24]. Despite promising initial results of EEN in management of adult CD, there is no data on use of EEN in refractory CD from India. We report our experience on use of 12-week EEN in adult CD refractory to anti-TNF agents.
METHODS
1. Study Design
This is a retrospective analysis of adult patients (age >18 years) with anti-TNF refractory CD who received EEN for induction of remission at Dayanand Medical College and Hospital, Ludhiana, India, between April 2018 and March 2019. The study was approved by the Institutional Review Board of Dayanand Medical College and Hospital (IRB No. DMCH/R&D/2020455) and performed in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all the participants.
2. Study Population
Adult patients (age >18 years) with moderate to severe active (CDAI >220), refractory (i.e., primary or secondary nonresponse and/or intolerance to anti-TNF agents [infliximab or adalimumab biosimilar], Supplementary Material 1) [6] CD, and on stable dose of 5-ASA (5-aminosalicylic acid; 3–4.8 g/day) and/or azathioprine (1.5–2 mg/kg/day) for 12 weeks with a 4- to 8-week interval between last dose of anti-TNF and study enrolment, were offered EEN. The diagnosis and classification of CD had been made as per established international criteria based on combination of clinical, endoscopic, histological, radiological, and/or biochemical investigations [25,26]. Presence of fistula, if any, was confirmed by physical examination, colonoscopy, examination under anesthesia, CT and/or magnetic resonance (MR) enterography.
A commercially available preparation (Ensure Plus Peptide; Abbott Laboratories, Zwolle, the Netherlands) (Supplementary Table 1) was used for EEN, targeting 35 kcal/kg ideal body weight (IBW) and 1.5 g protein/kg IBW, divided into 7–8 oral meals per day for 12 weeks. No table food was allowed except for drinking water. Standard of care treatment including 5-ASA, thiopurines and biologics (except in primary nonresponders and intolerants) were continued and corticosteroids were tapered as scheduled. An IBD counsellor frequently contacted the patients to ensure adherence to both pharmacological agents as well as EEN.
3. Outcomes
Primary outcomes included achievement of clinical remission and fistula healing at 12 weeks (in patients who had a documented fistula). Disease activity was assessed by CDAI and Perianal Crohn’s Disease Activity Index (PDAI) at baseline, week 8, and week 12. CDAI <150 was defined as clinical remission, whereas an improvement of ≥100 points was taken as response [27]. Efficacy in fistula healing was measured by Fistula Drainage Assessment in terms of response (a reduction in fistula drainage of 50% or more) and remission (complete cessation of fistula drainage for at least 4 weeks). Percentage reduction of the fistula drainage was indirectly measured by the frequency of having to change sanitary pads or dressing gauzes. Loss of response was defined by the recrudescence of the draining fistula [28]. Improvement in inflammatory markers (high sensitivity CRP [hs-CRP] and and ESR) and nutritional status (BMI, serum albumin, and hemoglobin) were the secondary end points.
4. Statistical Analysis
All analyses were performed using SPSS version 21.0 software (IBM Corp., Armonk, NY, USA). Quantitative data were expressed as mean±SD. Proportionate data was expressed in percentages. The Student t-test or Pearson chi-square test was used to compare values of index before and after EEN. P<0.05 was considered statistically significant.
RESULTS
A total of 130 adult patients with CD attended gastroenterology clinic between April 2018 and March 2019 and 23 received antiTNF (infliximab [n=9] and adalimumab biosimilar [n=14]). Out of these 7 patients (30.4%) had anti-TNF refractory CD and were offered EEN. Six patients (66.7% of females; mean age, 25.6±6.5 years) consented and were included in the study (Fig. 1). The median interval between reception of last dose of anti-TNF agent and study enrolment were 4 weeks. Calorie and protein requirements were calculated for each patient and EEN formulation and dosage was individualized (Supplementary Table 2). Baseline demographics of these patients are outlined in Table 1.
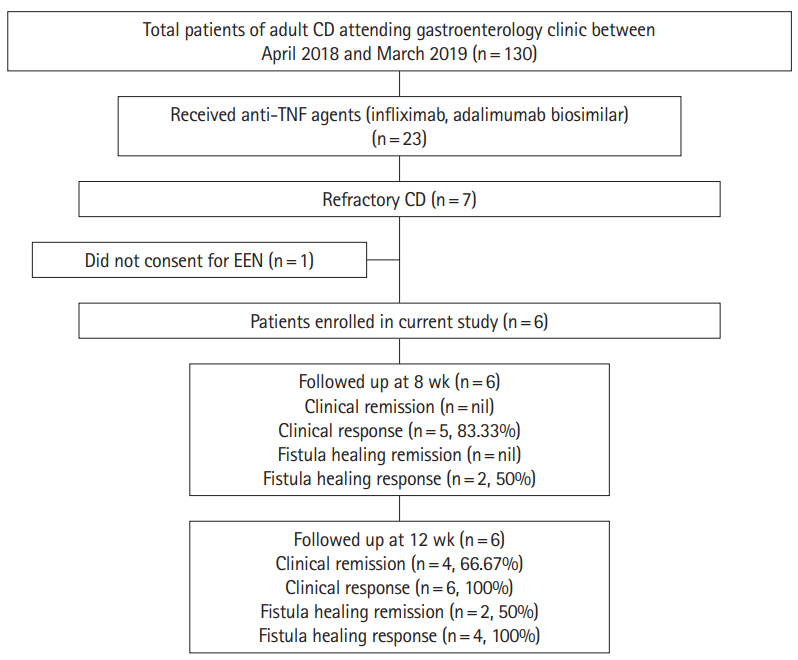
Flow of patients in current study. EEN, exclusive enteral nutrition.

Baseline Demographics of the Enrolled Patients (n=6)
1. Clinical Remission and Fistula Healing at 8 and 12 Weeks
1) Week 8
Clinical response (CDAI decreased by >100) was seen in 5 patients (83.3%) at week 8, though none achieved clinical remission (Table 2). Assessment of perianal fistula showed a reduction in fistula drainage of 50% or more (clinical response) in both the patients with perianal disease. Entero-enteric fistulas (n=2) were not assessed at week 8.

Disease Activity Parameters on EEN (n=6)
2) Week 12
All patients (100%) completed 12-week EEN and achieved clinical response. Four patients (66.6%) achieved primary end point of clinical remission (CDAI <150). Mean CDAI of patients decreased significantly after 12 weeks of EEN (388.8±74.8 vs. 160.0±25.2, P<0.001).
PDAI decreased to <10 in both the patients with perianal fistula (Table 2). Fistula disease assessment for perianal fistulas showed persistent clinical response in both the patients, though none achieved remission. Two patients had enteroenteric fistulae at baseline. Follow up MR enterography at 12 weeks showed complete healing of fistula in both the patients.
2. Assessment of Inflammatory and Nutritional Parameters at 8 and 12 Weeks
1) Week 8
We observed a significant decline in both mean hs-CRP (26.2± 13.8 mg/L vs. 19.7±10.3 mg/L) and mean ESR (45.5±10.9 mm/ hr vs. 31.2±7.9 mm/hr) after EEN at week 8 (P=0.01 and P=0.003, respectively). The average BMI also improved after EEN (15.6± 3.1 kg/m2 vs. 18.1±2.4 kg/m2, P=0.002). Other nutritional indices (hemoglobin: 8.2±1.1 g/dL vs. 10.6±0.8 g/dL and serum albumin: 2.8±0.3 g/dL vs. 3.1±0.2 g/dL) also showed significant improvement after EEN at week 8 (P=0.006 and P=0.02, respectively) (Table 3, Fig. 2).
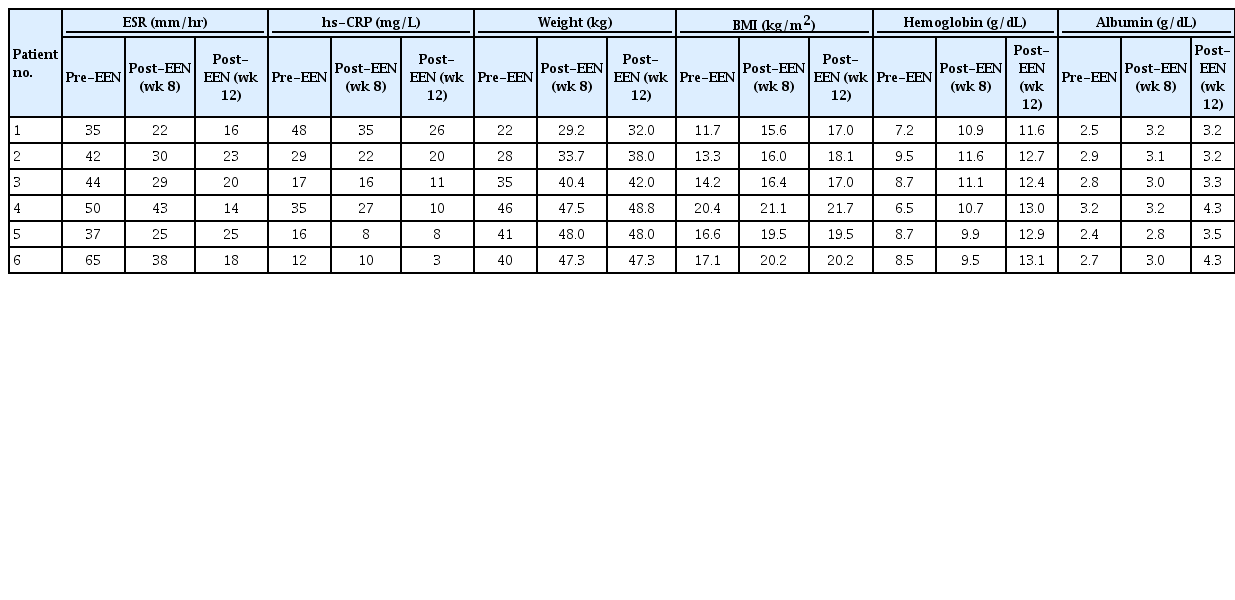
Inflammatory Markers and Nutritional Status on EEN
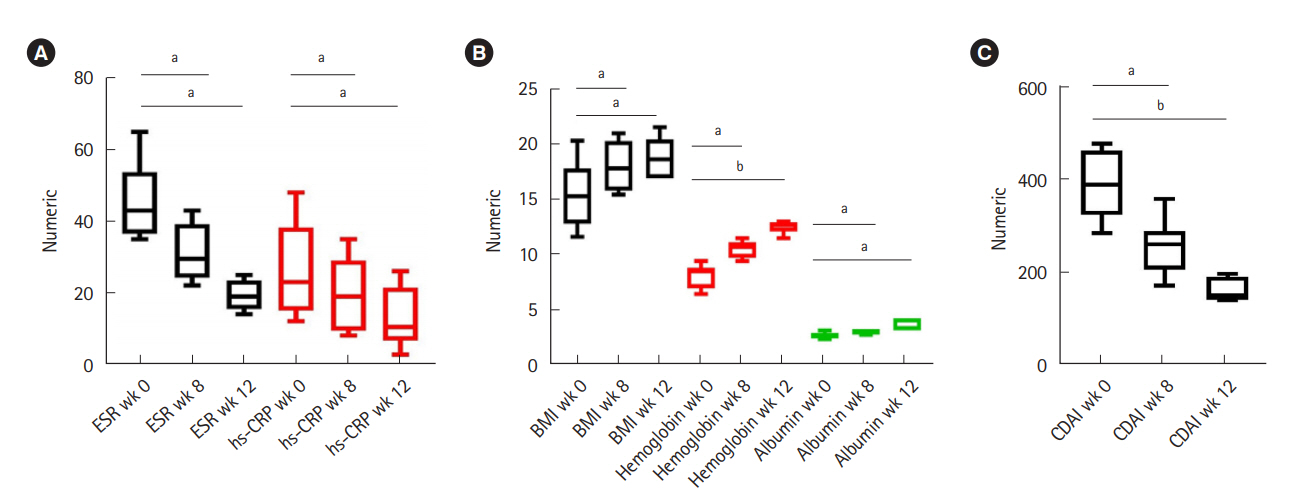
Trends in inflammatory markers (A), nutritional status with exclusive enteral nutrition (B), and CDAI (C). aP<0.05; bP<0.001. hsCRP, high sensitivity CRP.
2) Week 12
The improvement in inflammatory markers (hs-CRP and ESR) persisted in all the patients till week 12. The mean BMI improved from 15.6±3.1 kg/m2 at baseline to 18.9±1.9 kg/m2 post 12-week EEN. Similarly, hemoglobin and serum albumin also improved significantly from 8.2±1.1 g/dL and 2.8±0.3 g/dL at baseline to 12.6±0.6 g/dL and 3.6±0.5 g/dL post-EEN respectively (P<0.001 and P=0.006, respectively) (Table 3, Fig. 2).
3. Tolerability and Adverse Events
All 6 patients (100%) completed 12 weeks of EEN. None of the patients were intolerant to EEN and none had worsening of disease activity or needed emergency surgical intervention.
There were no withdrawals due to adverse events though mild nausea, vomiting, heartburn, flatulence and abdominal bloating were complained by all the patients. However, these were transient, observed in first 2 weeks of EEN, and improved subsequently. No serious adverse events were noted.
DISCUSSION
Globally, few studies have reported therapeutic benefit of EEN for induction of remission in adults with inflammatory/stricturing/fistulizing CD but none of these have evaluated its role in refractory CD [18-24,29]. This is the first account of effects of EEN, used as a salvage therapy, in adults with anti-TNF refractory CD from India.
EEN could induce remission in 66.67% patients at week 12. Disease activity indices (CDAI and PDAI) and inflammatory markers (ESR and hs-CRP) improved in all the 6 patients (Fig. 2). Entero-enteric fistulae showed complete radiologic remission at 12 weeks whereas refractory perianal fistulae showed improvement in Fistula Drainage Assessment as drainage decreased by >50% in both the patients, though none achieved complete remission. Nutritional status (BMI, hemoglobin, and serum albumin) also improved in all the patients post-EEN (Fig. 2B).
Interactions between diet and gut microbiota shape host immune responses. By eliminating various dietary components that can potentially compromise intestinal epithelial barrier and increase bacterial penetration to facilitate pro-inflammatory cascade, EEN confers a therapeutic benefit [30]. Its prebiotic properties also alter the metabolism of colonic microbiota [31]. The anti-inflammatory effects exerted by EEN could be attributed to the direct immunosuppressive effect or to modification of intracellular signaling pathways influencing the pro-inflammatory gene expression [32,33]. The attenuated production of cytokines decreases the mucosal inflammatory cytokine burden and promotes mucosal healing. It is also plausible that these immunomodulatory effects are mediated through the nutritional components (notably amino acids and vitamin D) of enteral formulae [34]. Decreased intensity of the inflammation as well as improved energy intake contributed to the observed increase in weight, BMI and other nutritional parameters.
Disease location is considered an important factor determining response to EEN [35,36]. Because all patients in the current study had ileo-colonic disease (L3), location specific effects with EEN could not be discerned. Encouraging rates of achievement of clinical remission in current study could also be ascribed to concomitant use of immunomodulators in all (100%) the patients. Moreover, 75% (n=3) of the patients who achieved clinical remission (n=4) received anti-TNF agents in combination with EEN. This is in synchrony with previously published data that demonstrates superiority of enteral nutrition therapy in combination with infliximab at not only inducing but also maintaining clinical remission in patients with CD as compared to infliximab monotherapy [37-40]. The combination therapy might act via magnifying the immunomodulatory effects of either of the agents. We did not assess EEN for maintenance of remission, though all patients enrolled in the current study are being continued on partial enteral nutrition after 12 weeks of EEN. We used a semi-elemental formula in the current study. The sources of proteins, fats and carbohydrates were whey protein concentrate, medium chain triglyceride oil and maltodextrins/sucrose respectively. A Cochrane review of 13 trials compared different formulations of enteral nutrition and found no difference in remission rates between different formulations. Similarly, source of proteins and fat in the formulae were unlikely to influence the therapeutic efficacy [41].
Despite the evidence for EEN being an effective strategy for inducing remission and promoting fistula closure in adult CD, it is underutilized in India. The main reasons for not using EEN remain high cost of therapy, availability and palatability of EEN formulations and limited availability of trained nutritionists. The cost of therapy in India is approximately INR 1,500–3,000 per day. Therefore a 12-week induction regimen with EEN will cost approximately INR 120,000 and 240,000 (USD, 1,700–3,500) depending on the nutritional requirements.
We acknowledge the limitations of our study. It is a retrospective, single-center study with small number of patients and lacks gut microbiome analysis. Also, we did not examine endoscopic findings, cross sectional imaging and fecal calprotectin. Nevertheless, EEN appears to be an attractive, effective and well tolerated therapy for induction of remission and improving nutritional status in anti-TNF refractory adult CD. More data from prospective trials with larger number of patients is required.
Notes
FINANCIAL SUPPORT
The authors received no financial support for the research, authorship, and/or publication of this article.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTION
Conceptualization and methodology: Sood A, Midha V. Formal analysis: Sood A, Singh A. Project administration: Sood A, Singh A, Midha V. Visualization: Sood A, Singh A, Sudhakar R, Midha V. Writing original draft: Sood A, Singh A, Sudhakar R. Writing review and editing: Sood A, Singh A, Sudhakar R, Midha V, Mahajan R, Mehta V, Gupta YK, Kaur K. Approval of final manuscript: all authors.
Supplementary Materials
Supplementary materials are available at the Intestinal Research website (https://www.irjournal.org).
Supplementary Material 1.
Refractory CD criteria.
Supplementary Table 1.
Ingredients of Commercially Available Preparation Used as Exclusive Enteral Nutrition
Supplementary Table 2.
Nutritional Value of Exclusive Enteral Nutrition (per Day)