Differences in the public medical insurance systems for inflammatory bowel disease treatment in Asian countries
Article information
Abstract
Background/Aims
The cost of caring for patients with inflammatory bowel disease (IBD) is high. Without government support, the cost burden will unavoidably rest on the patients and their family. However, the government providing full support will place a large financial burden on the health-care systems of a country. The aim of this study is to understand the current status of public medical insurance systems in caring for IBD patients among Asian countries.
Methods
Questionnaires inquiring about the availability of public health systems; medical, diagnostic, and endoscopy costs; and coverage rate of biologics use were designed and sent to IBD experts in each of the Asian countries studied. The results were summarized according to the feedback from the responders.
Results
The public health insurance coverage rate is high in Taiwan, Japan, South Korea, China, Hong Kong, and Singapore; but low in Malaysia and India. This probably affected the use of expensive medications mostly, such as biologics, as we found that the percentage of Crohn's disease (CD) treated with biologics were as high as 30%–40% in Japan, where the government covers all expenses for IBD patients. In India, the percentage maybe as low as 1% for CD patients, most of whom need to pay for the biologics themselves.
Conclusions
There were differences in the public health insurance systems among the Asian countries studied. This reportprovidesthe background information to understand the differences in the treatment of IBD patients among Asian countries.
INTRODUCTION
Inflammatory bowel diseases (IBDs) are chronic disabling gastrointestinal disorders affecting every aspect of the affected person's life, and account for substantial costs to the health-care system and society.1 With the growing number of patients with IBD and cases of hospitalization, the overall medical care cost consequently increases considerably. The annual hospitalization cost per patient, cost per hospitalization, and daily cost during hospitalization have increased significantly in the past decade (all P <0.001).2 The increased hospitalization costs of IBD patients may be associated with biologics use, length of hospital stay, medical insurance, subtypes of IBD, prognostic factors, surgery, and endoscopy.2
The cost of caring for IBD patients is high, with the annual mean cost of around US $6,000 to US $8,000 for CD patients, and US $4,000 to US $5,000 for UC patients in Germany (2006–2007) and the United States (2003–2004).34 Results from a large European inception cohort study, enrolling 1,321 patients with IBD diagnosed from October 1991 to September 1993, showed that the mean annual total expenditure on health care was €1,871 per patient-year (equating to approximately US $2,476 per patient-year) for IBD.5 The most expensive aspects were medical and surgical hospitalizations, together accounting for 63% of the cost in CD and 45% in UC.
Recent studies demonstrated that the use of anti–tumor necrosis factor (TNF) therapy may be associated with a reduced need for surgery and hospitalization, as well as an improvement in the quality of life and work productivity in both CD and UC patients.6 There is an apparent shift in cost profile from surgery and hospitalization toward anti-TNF treatment; however, the relatively consistent overall costs suggest that the high costs of these drugs are partly compensated for by a reduction in surgery and hospitalization rates.
Without government support, the cost burden of caring for IBD patients will unavoidably rest on the patients and their family. However, if the government will provide full support, it will place a large financial burden on the health-care systems of the country. With the increasing incidence and prevalence of IBD, as well as the use of more and more biologics and state-of-the-art techniques in treating or monitoring IBD patients, how and to what extent public medical insurance support affects current IBD management becomes a practical issue. In this report, we compare the differences in public medical insurance systems for IBD patients among Asian countries, and try to build a basis for understanding the differences and limitations in treating IBD patients among different countries.
METHODS
Questionnaires were designed to gather (i) general, (ii) diagnosis, (iii) treatment, (iv) disease monitoring, and (v) management information, as well as to inquire about the availability of public health systems, the costs of medical, diagnostic, and endoscopy expense, and the coverage rate of biologics use. The questionnaires were sent to IBD experts in each of the Asian countries studied. The results were summarized according to feedback from the responders. The summarized results were returned for review and approval by the responding IBD experts from each country.
RESULTS
We collected responses from Japan (Dr. Tadakazu Hisamatzu), South Korea (Dr. Hyun-Soo Kim), China (Dr. Bayasi Guleng), Hong Kong (Dr. Siew C. Ng), Singapore (Dr. Khoon Lin Ling), Malaysia (Dr. Ida Hilmi), and India (Dr. Vineet Ahuja) in June 2014. The responses were combined with the results from Taiwan, and summarized as the overall results for this report.
1. General Information
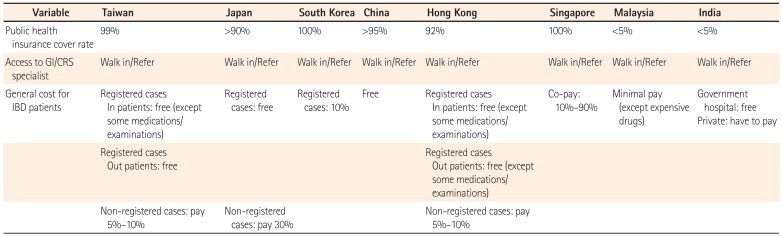
As shown in Table 1, the public health insurance coverage rate is high in Taiwan, Japan, South Korea, China, Hong Kong, and Singapore but low in Malaysia and India. Patients could consult a gastroenterologist or colorectal surgeon by either the walk-in or referral system for the diagnosis and treatment of their IBD in all of these countries. A registration system is available in Taiwan, Japan, South Korea, and Hong Kong. In these countries, registered IBD patients could obtain good support from the government, with their own expenses for treatment being zero (Japan) to minimal (Taiwan, South Korea, and Hong Kong). In Singapore, the copayment rate ranges from 10% to 90%. In Malaysia, payment for general care is low and does not include biologics. In India, most patients are treated in private service hospitals, with the patients themselves shouldering the entire medical expense.

General Information of the Public Health Insurance in Asia
2. Diagnosis
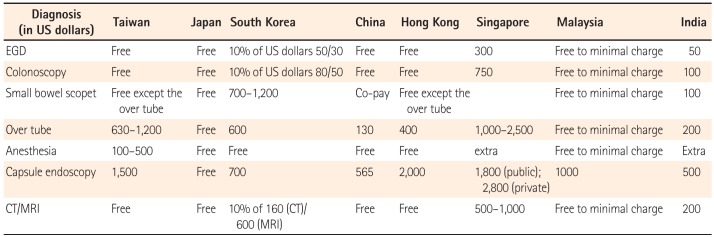
As shown in Table 2, among the diagnostic endoscopy methods, capsule endoscopy is the most expensive (from US $500 to US $2,800), except in Japan where the cost of capsule endoscopy is covered by the government. The most common tool for diagnosing IBD, ileocolonoscopy, was mostly free except in Singapore (about US $750) and India (about US $100).

Comparison of the Cost for IBD Diagnostic Tools in Asia
3. Treatment
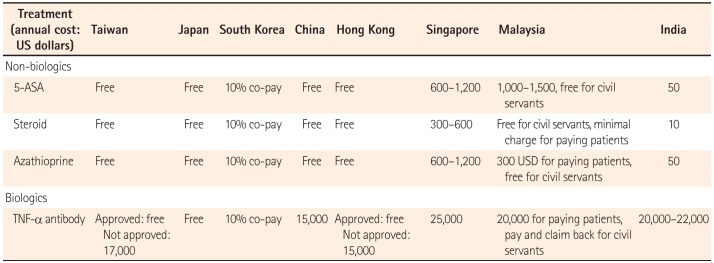
As summarized in Table 3, conventional therapies (5-aminosalicylic acid, steroid, immunomodulators) are paid for by public health insurance in Taiwan, Japan, China, and Hong Kong; in Korea, a 10% copayment system is established. Conventional therapies are paid for by patients in Singapore, Malaysia, and India, and the cost is higher in Singapore than in India. In Japan, biologics are paid for by the government, without a need for prior approval and without a time limitation. In South Korea, patients are responsible for a 10% copayment for biologics. In Taiwan and Hong Kong, the use of biologics needs to be approved in advance to be eligible for a reimbursement. Patients have to pay for biologics in China, Singapore, Malaysia (except civil servants), and India. The cost is between US $15,000 to US $25,000 per patient per year.
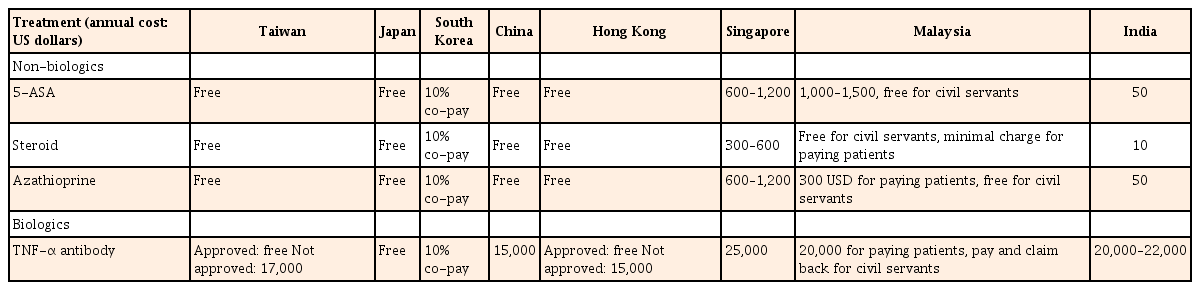
Comparison of the Cost for IBD Treatment in Asia
4. Monitoring
Tests for complete blood cell count, CRP, ESR, and serum biochemistry for the follow-up of IBD patients are covered by the government or minimally paid for by the patients in all of the countries studied (Table 4). Fecal calprotectin test is available in clinical practice in Singapore and India, costing about US $40 to US $80. It is available for research purposes in Taiwan, Japan, South Korea, and Malaysia; however, it is not yet available in China and Hong Kong. Tests for TNF-α antibody titer and the antibody to TNF-α antibody are not yet available in all these countries.

Comparison of the Cost for IBD Monitoring Tools in Asia
5. Risk Management
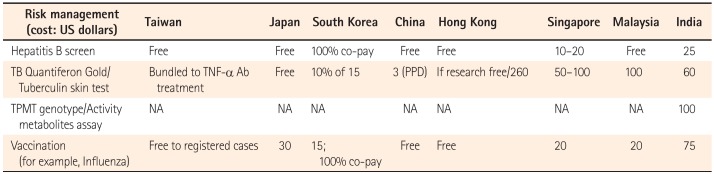
Hepatitis B screening is covered by public health insurance in Taiwan, Japan, China, Hong Kong, and Malaysia. In South Korea, Singapore, and India, patients themselves have to pay for hepatitis B screening (US $10–25). Mycobacterium tuberculosis screening and monitoring are bundled with TNF-α treatment in Taiwan; covered by the government in Japan; and paid for by patients in South Korea (10% copayment), China, Hong Kong, Singapore, Malaysia, and India (US $50–260). Thiopurine S-methyltransferase (TPMT) genotyping/activity and thiopurine metabolite assays are only available in India and cost about US $100. Vaccination programs are free for registered IBD patients in Taiwan, as well as in China and Hong Kong. In other countries, patients have to pay for vaccination (Table 5).

Comparison of the Cost for IBD Risk Management in Asia
6. Possible Impact
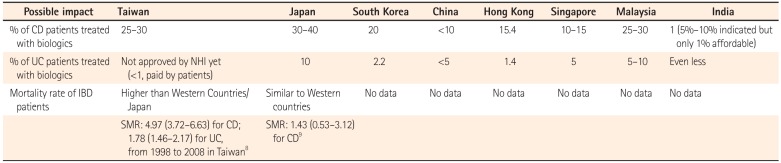
The above results are in line with the previous reports stating that the cost is mostly related to medical expenses, especially biologics. We hypothesized that the percentages of IBD patients taking biologics would be different between countries with a high and those with a low public health coverage. Indeed, we found that the percentage of CD patients treated with biologics was as high as 30%–40% in Japan, where the government covers all expenses for IBD patients. The percentage maybe as low as 1% for CD patients in India, where most of the patients have to pay for the biologics themselves (Table 6).

Possible Impacts Derived From the Differences of Public Health Insurance in Asia
As reports on mortality results are available only from Japan and Taiwan, and biologics only became available for clinical use in Taiwan in 2008, it might be too early to draw any conclusion about public health insurance–related mortality in IBD patients in these Asian countries.
DISCUSSION
From this survey, we found that there were differences in the public health insurance systems among Asian countries. This probably affected the proportion of patients who need to be treated with more expensive medications such as the biologics. Japan and India are the two extremes for this situation. The percentage of IBD patients taking biologics is highest in Japan, where the payment for the diagnosis, treatment, and monitoring of IBD is entirely covered by the government. In contrast, the percentage of IBD patients taking biologics is lowest in India, where the coverage rate by public health insurance is low and IBD patients have to pay for most of their medical expenses. As biologics have been proven to improve the clinical and mucosal status of IBD patients,7 determining whether the difference will affect the outcomes (such as operation rate, admission rate, or even mortality rate) needs a longer period of follow-up.
This report has some limitations. First, not all IBD experts in the Asian countries studied replied to the survey. Second, those who did reply were limited in number, and thus might not be representative of the true situation in each country. Third, no surgical rate, admission rate, and mortality results were available from all the countries. Therefore, this report could function as an initial report providing background information for understanding the differences in the treatment of IBD patients among countries in Asia.
In summary, this is the first report to compare the public health insurance systems in Asia, especially focusing on IBD-related diagnosis and treatment. The effect derived from the differences needs a longer period of observation to allow making a firm conclusion.
ACKNOWLEDGEMENT
The author would like to thanks to Dr. Tadakazu Hisamatzu, Dr. Hyun-Soo Kim, Dr. Bayasi Guleng, Dr. Siew C. Ng, Dr. Khoon Lin Ling, Dr. Ida Hilmi, Dr. Vineet Ahuja, and Dr. Chun Jen Ooi for their great input to this study.
Notes
Financial support: None.
Conflict of interest: None.