INTRODUCTION
Ulcerative colitis (UC) is a chronic relapsing and remitting inflammatory disease of the colorectum. Currently, there is no radical medication for UC, and the therapeutic goal is to maintain endoscopic remission [1]. Long-term inflammation is associated with an increased incidence of neoplasia [2], and there is growing interest in colitis-associated cancer (CAC), which has a significant prognostic impact [3], considering that advances in immunosuppressive therapies have reduced the overall likelihood of colectomy in patients with UC [4]. The characteristics of CAC are different from those of usual sporadic tumors because UC-associated neoplasms (UCANs) occur primarily via the p53-mediated oncogenic pathway [5]. Developing from flat areas with a variety of morphologies, UCAN often forms fields or occurs in multiple locations. Furthermore, it is known that the rare histologic subtypes of colorectal cancer, namely, poorly differentiated adenocarcinoma (por), signet-ring cell carcinoma (sig), and mucinous adenocarcinoma (muc), are relatively common in CAC, whereas most sporadic colorectal cancers are well to moderately differentiated tubular adenocarcinoma (tub) [6-9]. In the past, UCAN was treated in principle by pancolectomy. However, with advances in endoscopic diagnostics and therapeutics and publication of the SCENIC consensus statement [10], endoscopic resection (ER) has become an option. Nevertheless, the definition of lesions that are endoscopically resectable and the criteria for resection are unclear, and there is no mention of histologic subtypes [10-12]. The por/sig/muc component is considered a poor prognostic factor even in patients with sporadic tumors that are treated endoscopically [13,14]. However, the clinicohistolologic and endoscopic characteristics of UCAN containing a por/sig/muc component have rarely been documented. This study aimed to determine the prevalence of por/sig/muc component in UCAN and its association with invasiveness and to clarify its clinicohistologic and endoscopic features, including its detectability at the time of biopsy prior to resection.
METHODS
1. Patient Selection and Data Collection
The study had a retrospective observational design and included patients diagnosed with UC-associated high-grade dysplasia (HGD) or adenocarcinoma at the Division of Gastroenterology and Hepatology, Department of Internal Medicine, Keio University Hospital (Tokyo, Japan) between March 1997 and September 2022. Prognostic data, namely, information on deaths from colorectal cancer, were collected through to December 2022. This cohort includes previously reported cases of UCAN [15-18], which were identified endoscopically and confirmed histopathologically by at least 2 experienced pathologists who have expertise in UCAN, but does not include non-dysplastic lesions, neuroendocrine tumors, sporadic adenoma/carcinomas, serrated lesions, traditional serrated adenomas, or indefinite UCAN. UC-associated low-grade dysplasia finally diagnosed by resected specimen was also not included. Patients were excluded if they refused surgery or were referred to another hospital before surgery with an unknown course. Information was collected on patient demographic and disease characteristics, including sex, age at time of detection of UCAN, duration of UC, extent of disease, location of UCAN, and whether concomitant primary sclerosing cholangitis was present.
2. Definition and Evaluation of Endoscopic Findings
Neoplastic lesions were detected by targeted biopsies using a video colonoscope (GIF-XZ1200, PCF-H290ZI, PCF-Q260AZI, PCF-Q240ZI, CF-HQ290I, CF-H260AZI, CF-HQ260I, PCF-H290I, PCF-Q260AI, CF-H290I, CF-Q260AI, CF-H260AI, CF-Q240I, or GIF-XP260 [Olympus, Tokyo, Japan] or EC-L600ZP7 [Fujifilm, Tokyo, Japan]). Regular white-light colonoscopy was performed, followed by application of 0.1% to 0.2% indigo carmine dye spraying [15,18]. According to the SCENIC consensus statement, lesions that were assumed to be intramucosal or submucosal were classified as pedunculated, sessile, superficial elevated, flat, or depressed [10]. Tumor morphology was determined macroscopically based on endoscopic appearance, irrespective of histology, even if the lesion appeared to be early-stage but was found to be advanced cancer postoperatively. The endoscopic morphology and disease activity according to the Mayo endoscopic subscoring system [19] were retrospectively evaluated after confirmation by agreement of several endoscopists with experience in colonoscopy for at least 2,000 cases with UC.
3. Histopathologic Diagnoses
Tissue was obtained from the lesion by endoscopic targeted biopsy or from an endoscopically resected specimen, surgical specimen, and/or ascites. The final histologic diagnosis was based on histologic evaluation of the entire endoscopically or surgically resected lesion. The exceptions were patients who did not undergo resection because of disseminated advanced cancer, in whom biopsy specimens and ascites fluid were used for histological evaluation. The histologic diagnosis was confirmed by routine hematoxylin-eosin staining with consideration of the immunohistochemical expression patterns of p53 (diffuse/unique basal overexpression or complete loss) and Ki-67, and the presence of UC-associated inflammation/dysplasia in the surrounding lesions as previously described [15,16,20,21].
Based on the Japanese criteria by the Ministry of Health, Labour and Welfare, whereby neoplasms with nuclear and architectural abnormalities are diagnosed as intramucosal carcinoma regardless of their invasion status, the neoplastic component was classified as HGD, tub, por, sig, or muc. In other words, intramucosal non-invasive carcinoma, classified as HGD in Western countries, was also in part classified as tub. When a tumor contains more than one histological type of carcinoma, all the histological types were recorded in descending order of each type occupied [22]. Mixed lesions that were predominantly tub but contained a por/sig/muc component (e.g., tub > por) were included in the por/sig/muc group (Group P), as well as tumors with a predominant por/sig/muc component (e.g., por > tub). Grade of differentiation and TNM stage were assessed according to the Japanese Society for Cancer of the Colon and Rectum definitions [22]. In disseminated cases where surgery was not performed, tumor depth was classified as serosa in the presence of extramural invasion on computed tomography images and cancerous ascites. Although these histologic diagnoses were based on Japanese criteria, the interpretation of the analysis in this study, which focused on the por/sig/muc component and prognosis, does not differ from judgments based on Western criteria.
4. Statistical Analysis
Continuous variables are expressed as the median and interquartile range. Mayo endoscopic subscores are expressed as the mean ┬▒ standard deviation. Categorical variables are expressed as the percentage. Intergroup comparisons were made using the Pearson chi-square test or Fisher exact test. The cumulative survival rate was calculated using the Kaplan-Meier method and compared between groups using the log-rank test. Cancer-related deaths were included in the analysis of cumulative survival and non-cancer-related deaths were censored at the time of death. All statistical analyses were performed using JMP version 16.2.0 (SAS Institute Inc., Cary, NC, USA). Graphs were generated using GraphPad Prism version 9.5.1 (GraphPad Software Inc., San Diego, CA, USA). Two-sided P-values of < 0.05 were considered statistically significant.
RESULTS
1. Patient Profile
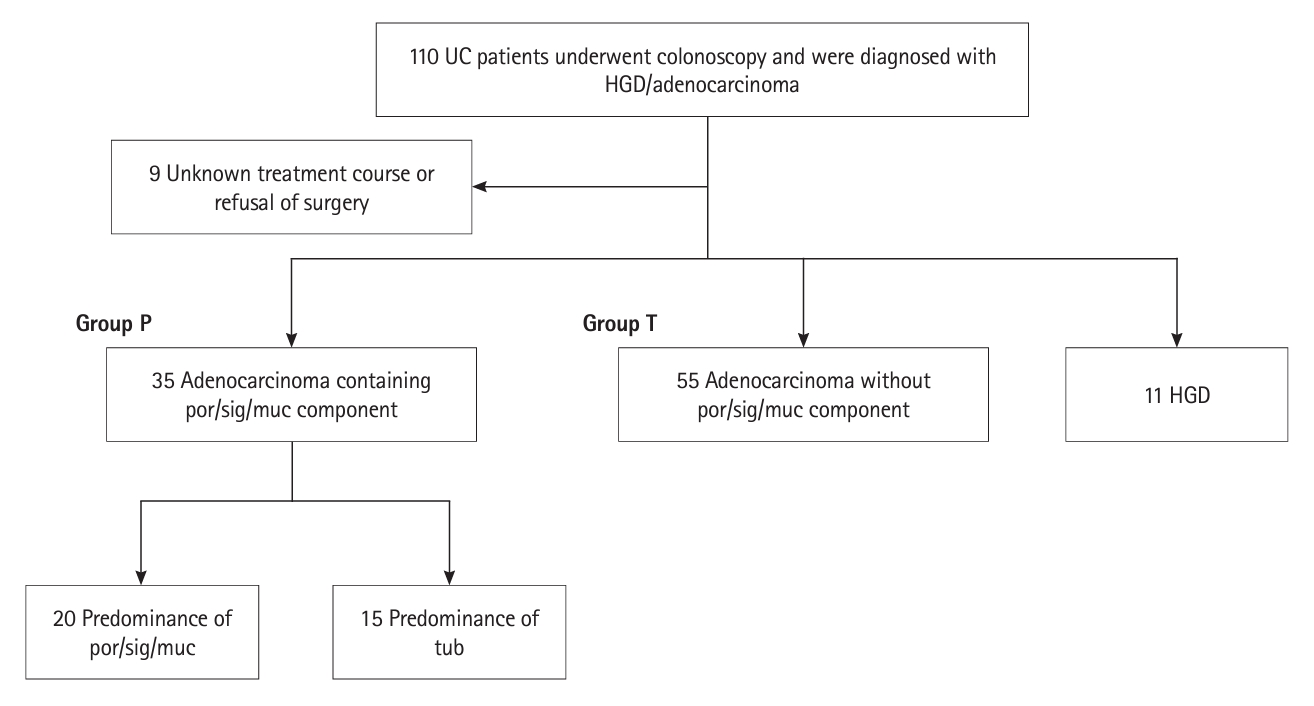
One hundred and ten patients who underwent colonoscopy at our institution between March 1997 and September 2022 were diagnosed with UC-associated HGD or adenocarcinoma. Nine patients were excluded because of refusal of surgery or an unknown treatment course after preoperative referral to other hospitals. A total of 140 lesions from the remaining 101 patients were analyzed. Based on the final histopathologic diagnosis, 66 patients (101 lesions) were diagnosed to have HGD or tub lesions without a por/sig/muc component. Thirty-five patients (39 lesions) were diagnosed to have lesions with a por/sig/muc component. Twenty of these 35 patients were diagnosed as por, sig, or muc with a predominant por/sig/muc component and 15 as tub with predominant tub containing a por/sig/muc component (Fig. 1). Five patients were deemed inoperable and not evaluated by resection specimens; all but one were in the predominant por/sig/muc group because only por/sig/muc was detected. Twenty-three patients had multiple lesions; the most advanced lesions in these patients, as reflected by disease stage, contained por/sig/muc components.
For subsequent analysis, we classified 11 and 55 patients without and 35 with por/sig/muc components into ŌĆ£HGD,ŌĆØ ŌĆ£tubŌĆØ (Group T) and ŌĆ£por/sig/mucŌĆØ (Group P) groups, respectively. The patient characteristics were comparable whether or not a por/sig/muc component was present (Table 1). As previously reported [15], approximately 80% of lesions in both groups occurred in the sigmoid colon or rectum (Table 2). These results are in contrast with reports elsewhere suggesting that sporadic por/sig/muc often occurs in the right-sided colon [8,23]. As expected from the aggressive infiltration signature of por/sig/muc, the por/sig/muc-containing lesions were relatively deep and non-polypoid or advanced cancerous lesions based on endoscopic morphology.
2. Impact on Survival
Having confirmed the invasiveness of the por/sig/muc component, we then investigated the difference in survival between the Group T and Group P. Overall, the survival rate was lower in the Group P (n = 35) than in the Group T (n = 55) (P=0.001), with respective 5-year survival rates of 67% and 96% (Fig. 2A). Given that this comparison ignored tumor depth and stage (Table 3), we examined the differences in survival by stage in the Group T and Group P. No patients with stage 0-II disease died during the observation period even in the Group P (Group T, n = 49; Group P, n = 19); however, deaths occurred in patients with stage III or higher disease, with no significant between-group difference in the death rate (P=0.661) (Fig. 2B and C). Thus, cancer stage significantly affected the prognosis (P<0.001), highlighting the importance of early detection of CAC.
Next, we compared the survival rates according to tumor depth, which is a prognostic factor. The survival rate was 100% for patients who had lesions with a depth (intramucosa-muscularis propria) corresponding to stage 0-I in the depth component of the TNM classification in both groups (Group T, n = 45; Group P, n = 13) and were distinguished from lesions deeper than the subserosa (Group T, n = 10; Group P, n = 22). Meanwhile, when progressive lesions deeper than the subserosa were compared between the 2 groups, there was no significant difference in survival (P=0.379) (Fig. 2D). These findings were similar to those by stage, suggesting that the more advanced lesions in the Group P contributed to the lower survival rate.
3. Difficulties in Biopsy-based Histologic Diagnosis
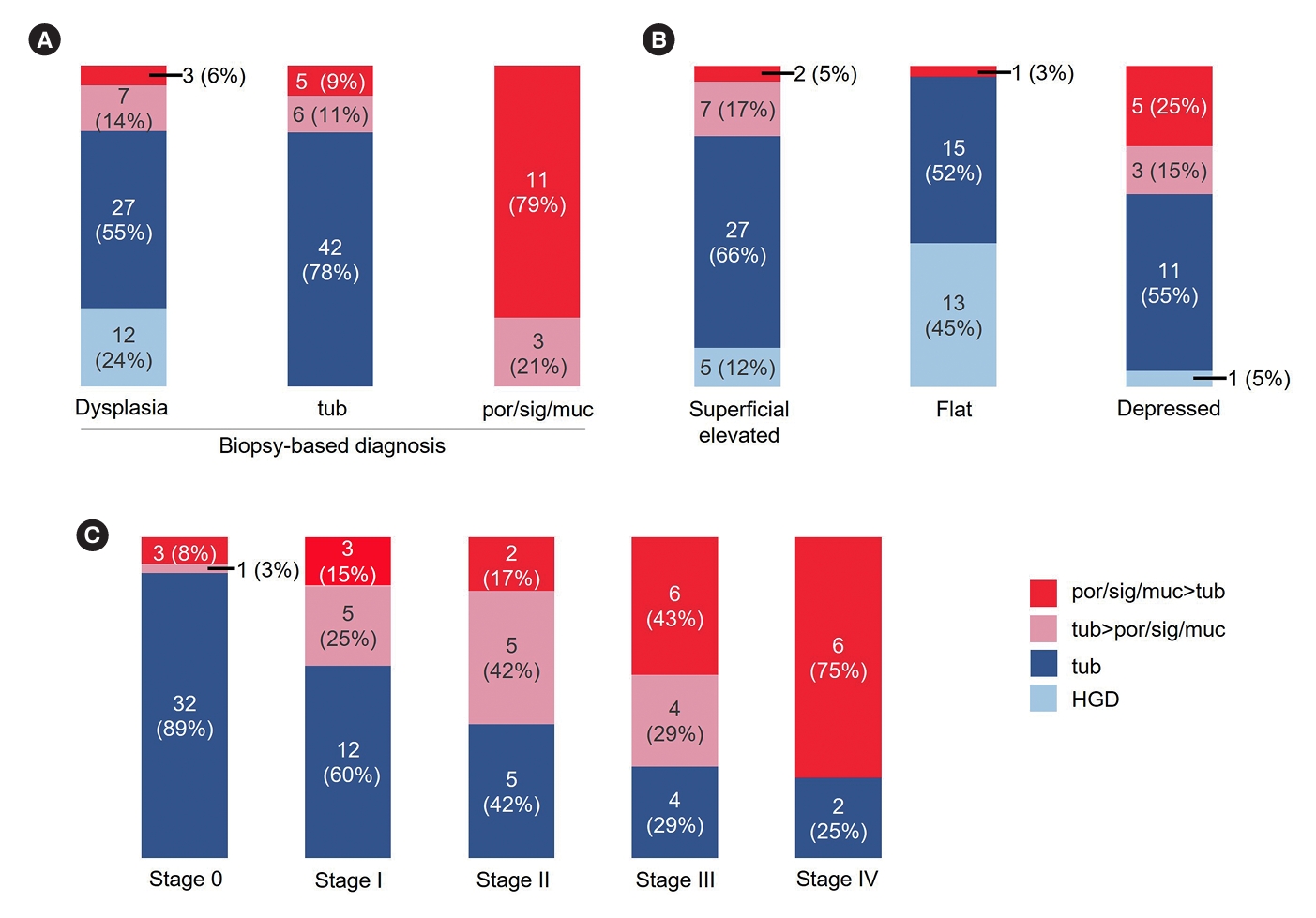
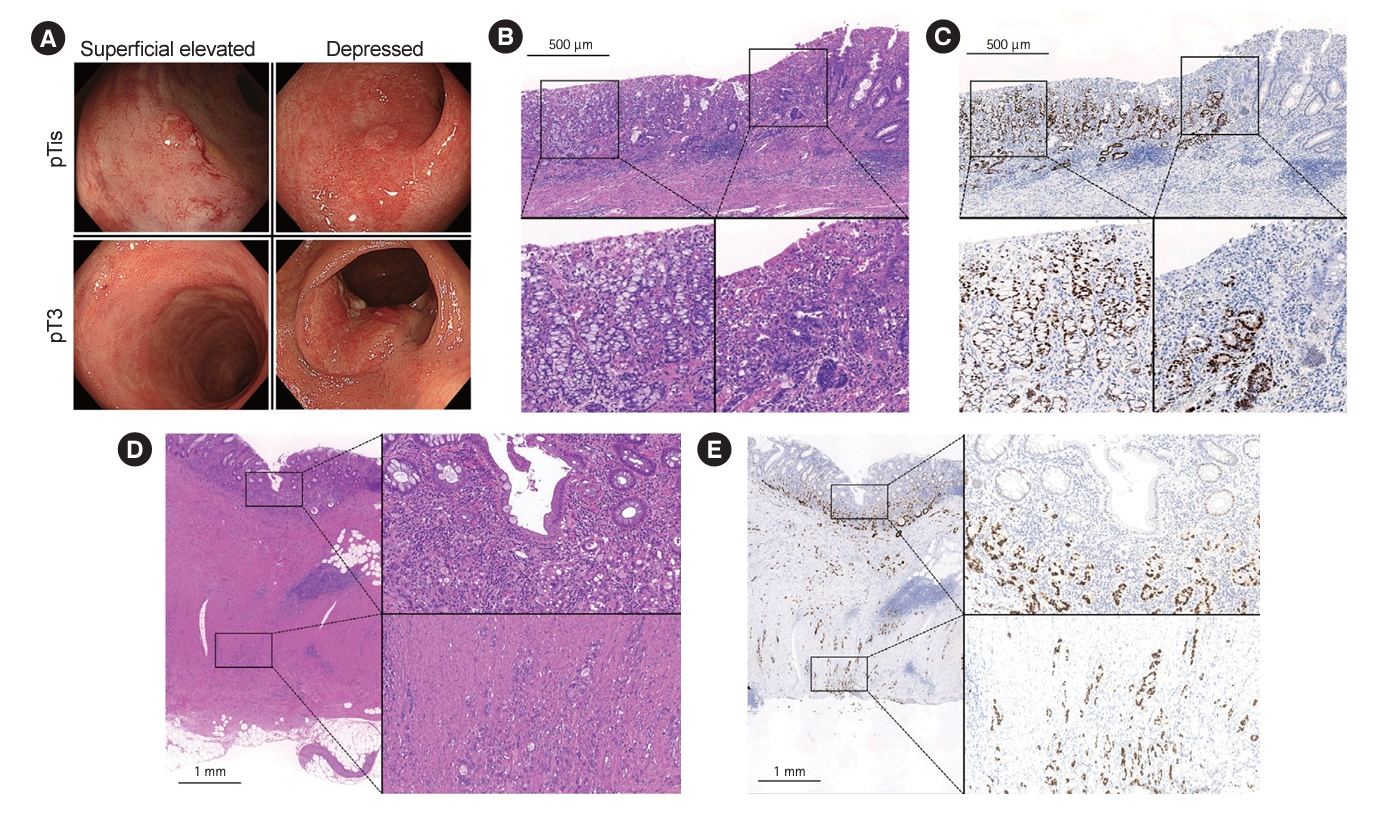
To determine whether the por/sig/muc component was recognized before selection of treatment, we evaluated the concordance of the histologic findings in cases of identifiable lesions in which both targeted biopsy and resection pathology information were available (n = 116). Unexpectedly, only 40% of lesions in Group P (14/35) had identifiable por/sig/muc components at the time of biopsy (Fig. 3A). The detection rate was not lower in cases without the use of a magnifying endoscope (56%; 5/9). Even when the por/sig/muc component was not detected on biopsy in patients with UCANs, the negative predictive value was 79% (81/102), meaning that 21% of the lesions might be false-negative even with a biopsy negative for por/sig/muc components. Representative images of tumor heterogeneity that may result in different histologic diagnoses for the same lesion depending on the biopsy site are shown in Fig. 4A-C. Focusing on the discrepancy between pre-resection and post-resection diagnoses in early-stage tumors, in our cohort of 78 UCAN cases with a tumor depth of intramucosa and submucosa, including HGD, 12 cases contained a por/sig/muc component but 50% (n = 6) were not detected by pre-resection biopsy.
Furthermore, CAC is associated with the difficulty of diagnosing the depth of cancer, as endoscopic findings may be classified as early-stage UCAN, but the depth of these cancers is often quite different (Fig. 4A). We examined whether the presence or absence of por/sig/muc differed in each category, even if the lesions were classified in the same category by endoscopic morphology according to the SCENIC classification. Importantly, a por/sig/muc component was noted in 0%, 0%, 22%, 3%, and 40% of pedunculated (0/4), sessile (0/13), superficial elevated (9/41), flat (1/29), and depressed (8/20) resected lesions, respectively, reflecting an infiltrative phenotype (Table 2, Fig. 3B). It should be noted that flat lesions are 0-IIb lesions that do not include flat elevated lesion, and por/sig/muc is extremely rare even among CAC in flat, sessile, and pedunculated lesions. Even if no por/sig/muc component was detected by biopsy, lesions with a depressed or superficial elevated surface may invade deeply, resulting in the presence of tumor components that cannot be recognized on intramucosal or submucosal examination alone (Fig. 4).
4. High Probability of por/sig/muc Components in UCAN
Given the expected increase in the proportion of por/sig/muc components detected due to tumor progression, we examined the proportions in each disease stage. Surprisingly, 11% (4/36) were found to be stage 0, 40% to be stage I (8/20), 58% to be stage II (7/12), 71% to be stage III (10/14), and 75% to be stage IV (6/8) (Fig. 3C). A high frequency of por/sig/muc components was found even in relatively early-stage tumors. When limited to tumors formally diagnosed as predominantly por/sig/muc, the proportions were 8% (3/36) for stage 0, 15% (3/20) for stage I, 17% (2/12) for stage II, 43% (6/14) for stage III, and 75% (6/8) for stage IV. When the mixed por/sig/muc component was considered, it became clear that the percentage was higher. Indeed, comparison of survival rates showed that the prognosis tended to be poorer in the por/sig/muc-predominant group than in the tub-predominant group (P=0.071). Although we could not show a statistically significant difference or correlation in the depth distribution between the 2 groups (P=0.537) because of the small sample size, the prevalence of subserosal or deeper invasion tended to be higher in the por/sig/muc-predominant group (por/sig/muc > tub [14/20] than in the tub > por/sig/muc group [8/15]).
DISCUSSION
Using endoscopic and histologic analysis, we have demonstrated that CAC containing a por/sig/muc component is invasive and has a poor prognosis. We first revealed that this component is often undetectable on biopsy before treatment selection. Our results suggest that despite the presence of por/sig/muc components in CAC from an early stage, a diagnosis based only on predominant components may underestimate the risk of the invasive potential of UCAN because of intratumoral cellular heterogeneity and extensive tumor formation. We believe that surveillance strategies and choice of treatment for UCAN should be based on a rigorous understanding of the nature of this type of neoplasia.
Patients with UC develop CAC as a result of accumulation of acquired somatic mutations in the colon that stem from previous bouts of severe inflammation [17,24], and the inflammation-related carcinogenesis result in characteristics that are fundamentally different from those of sporadic neoplasia [5]. Compared with sporadic neoplasms, UCAN has a younger age of onset and lesions often occur simultaneously. Importantly, UCAN often presents with an uncommon histologic subtype of colorectal cancer such as por/sig/muc [9]. Approximately 20% of CACs have been reported to be por/sig/muc [9], but we found that UCANs containing por/sig/muc components are much more common. We believe that more should be known about lesions containing por/sig/muc, which are considered to have the worst prognosis, when selecting treatment for UCAN.
Recent guidelines recommend ER as a treatment option for polypoid dysplastic lesions that can be resected completely en bloc unless multifocal or invisible dysplasia is found elsewhere in the colon. Compared with polypoid lesions, non-polypoid and invisible lesions have been shown to be at risk for progression to advanced cancer [25], which is consistent with the fact that all tumors containing por/sig/muc in this study were nonpolypoid lesions. Nevertheless, even selected non-polypoid lesions without stigmata of advanced cancer are considered acceptable for ER by experienced endoscopists [11,12]. Tubular adenomas, traditional serrated adenomas, and sessile serrated lesions also occur within the mucosa affected by UC. The causal association between these lesions and intestinal inflammation is difficult to define, and some consider all tumors that occur within the affected area to be UCAN [26]. Indeed, ER of well-defined tubular adenomas and large laterally spreading tumors without flat areas within the mucosa affected by UC can often be successfully managed without recurrence. The probability of high-risk UCAN with surrounding p53-mediated flat dysplasia may have been underestimated because the proportion of such tumors in the total tumor population is low when combined with the relatively low-risk tumors with demarcated borders that occur in the mucosa in patients with UC.
UCANs often exhibit extensive flat morphology with heterogeneity, resulting in tumors that have a por/sig/muc component in a small portion being classified as tub when evaluated in their entirety. As the poor prognostic properties, we used the presence or absence of the por/sig/muc component in this classification method. The risk of por/sig/muc may have been underestimated in relatively early CAC lesions because of their unique developmental morphology. It has been reported that CAC tends to be more poorly differentiated when the carcinoma invaded the submucosa or deeper in comparison between the surface and deep parts of the lesions [27]. A noteworthy finding in this study was that, in addition to the high por/sig/muc rate in advanced cancers, a relatively high percentage of por/sig/muc components were detected in early-stage cancers, with 11% in mucosa and 40% in submucosa. Even if biopsy was performed, our detection rate of por/sig/muc components was low. Although we cannot directly discuss ER, given that most lesions in our cohort were surgically resected, we should be very cautious about performing ER for tumors in patients with UC, considering that UCAN often contains a por/sig/muc component. At the very least, we believe it is essential to avoid resections that obscure the margins, such as cold snare polypectomy, and to evaluate the resected specimens for negative margins, including p53 immunostaining. After complete histologic resection in patients with HGD, follow-up with surveillance colonoscopy may be feasible in most cases [28]. However, histopathologic diagnosis, which is limited to evaluation of a section of a specimen, does not exclude the chance of a remnant tumor cell. It is important to make appropriate surgical treatment choices because early and complete resection is curative and has a good prognosis, even if there is a por/sig/muc component.
This study had some limitations. First, it involved retrospective collection of descriptive data for a small number of subjects from a single center and we were unable to examine the data in multivariate analysis because of the small number of deaths. Therefore, more subjects are needed to confirm our findings. Endoscopic equipment, imaging methods, intervals of examination, and biopsy methods have not been standardized, but this is because this study was based on long-term real-world data. However, this is the first and largest study to report such findings and was conducted at a high-volume center that more than 3,000 patients with inflammatory bowel disease attend annually. No other published studies have included such a detailed analysis of endoscopic and histologic images or determined the prognosis of UCAN with por/sig/muc components, including early and advanced cases, because of the difficulty of detecting UCAN in its early stages. Second, we were unable to perform molecular genetic and epigenetic investigations. Histopathologic diagnosis of UCAN was determined in this cohort primarily by p53 abnormalities based on immunohistochemistry, which may not have been able to discriminate advanced sporadic tumors unrelated to inflammation that occurred within the affected area. It also does not provide any evidence that would indicate whether the por/sig/muc component of UCAN appeared as a consequence of progression or a cause of progression. Third, the data in this study may be affected by the selection bias because many of the study participants were high-risk cases for which surgery was indicated. This is not a study of low-grade dysplasia, which is more likely to be resected endoscopically.
In conclusion, our findings highlight the risk of a por/sig/muc component in UCAN. This risk may have been underestimated and its presence may not be detected by biopsy before resection because of intratumoral heterogeneity. Considering that the prognosis may be poorer for CAC than for sporadic tumors, it is important to carefully determine the indications for ER in patients with UC, even for tumors that appear to be endoscopically resectable.