INTRODUCTION
Small bowel cancers are very rare, accounting for only 3%-6% of all gastrointestinal neoplasms.1,2 Because small bowel cancers lack specific clinical manifestations, and the entire small intestine is not easy to access, it is very difficult to diagnose cancers in this region.
The development of balloon-assisted enteroscopy (BAE) and capsule endoscopy has initiated a new era in small bowel lesion diagnosis. BAE is a relatively noninvasive method compared to surgical resection, with a diagnostic yield of approximately 43%-80% for small bowel diseases.3 BAE has advantages over other diagnostic modalities such as capsule endoscopy, not only in terms of access to the entire small bowel with real-time observation, but also in facilitating endoscopic intervention, tissue confirmation with biopsy, and procedures such as stenting and balloon dilatation.4,5,6
Here, we report a case of small bowel metastatic carcinoma observed with double balloon enteroscopy (DBE) in a patient with a history of multiple cancers.
CASE REPORT
A 69-year-old woman was referred to our clinic complaining of cramping abdominal pain that had persisted for 10 days and had been aggravated for one day before admission due to a small bowel obstruction. She had a history of multiple cancers including ovarian cancer (treated by total abdominal hysterectomy and bilateral salpingo-oophorectomy 12 years prior), bladder cancer (treated by transurethral resection of the bladder tumor 5 years prior), and breast cancer (treated by left modified radical mastectomy followed by adjuvant chemotherapy 6 years prior). On admission, her blood pressure was 110/70 mmHg, heart rate was 92 beats/min, body temperature was 36.4Ōäā, and respiratory rate was 20 breaths/min. Laboratory data revealed anemia (white blood cells, 8,100/mm3; hemoglobin, 8.0 g/dL; platelets 297,000/mm3), and biochemical tests revealed no abnormal findings (CRP, 4.18 mg/L; glucose 162 mg/dL; BUN, 11.6 mg/dL; creatinine, 0.73 mg/dL; AST, 20 IU/L; ALT, 13 IU/L; total bilirubin, 0.48 mg/dL; protein, 7.2 g/dL; albumin, 4.0 g/dL; PT, 13.3 seconds [International Normalized Ratio 1.0], and aPTT, 29.7 seconds). Urinalysis did not reveal any abnormalities.
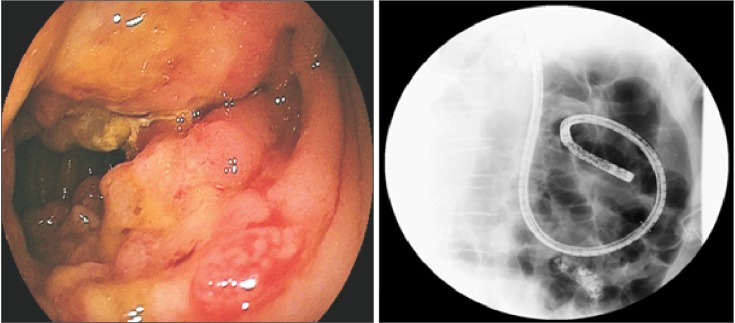
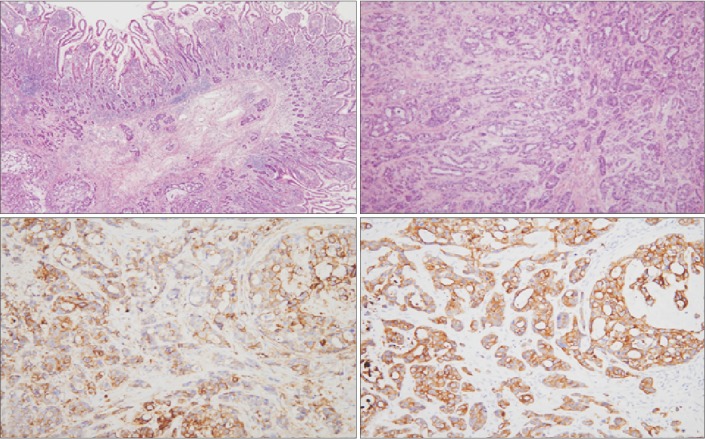
Neither esophagogastroduodenoscopy nor colonoscopy revealed any specific findings. Conventional abdominal CT scans revealed a circumferential wall-thickening lesion in the proximal to mid jejunum, and because the patient had a history of multiple cancers, this lesion was treated as suspicious and assumed to represent metastatic small bowel cancer or (less likely) adenocarcinoma (Fig. 1A, B). A fluoroscopic small bowel follow-through revealed a 2-cm circumferential wall-thickening lesion appearing as an "apple core sign" in the mid jejunum (Fig. 1C). For pathological confirmation, antegrade DBE (EN450T5, Fujinon, Saitama, Japan) was performed under conscious sedation. An approximately 2-cm long encircling ulcero-infiltrative lesion was noted at the mid jejunum (depth of insertion approximately 100 cm) with partial luminal obstruction (Fig. 2). The total procedure time was approximately 50 minutes. Two pieces of tissue were biopsied, and histological examination revealed atypical epithelial nests with nuclear pleomorphism and frequent mitosis (Fig. 3); the biopsy result was strongly suggestive of metastatic breast cancer. The patient underwent small bowel resection for her continuing abdominal pain, and the final pathological diagnosis was small bowel metastatic carcinoma originating from the breast (Fig. 4). The patient underwent chemotherapy in the oncology department, and we administered docetaxel monotherapy, the most common drug for the treatment of breast cancer (75 mg/m2 on day 1, 21 days for 1 cycle). Following 6 cycles of chemotherapy, new metastatic lesions in the brain were observed, and brain radiotherapy was performed 1 year after diagnosis. Three years have passed since the initial diagnosis. No remnant lesions or new lesions have been found, and the patients visited the hospital every 3 months for follow-up investigations under good conditions.
DISCUSSION
Since the introduction of DBE, small bowel tumors can be easily diagnosed without surgical resection, and several studies have reported the characteristics of diagnosing small bowel tumors using DBE. Recent studies concerning small bowel tumors using DBE have shown that the most common type of small bowel carcinoma is metastatic small bowel cancer followed by adenocarcinoma, carcinoid tumors, and lymphoma.1,3
Metastatic small bowel cancer is more frequent than primary small bowel cancer. However, the overall incidence of metastatic small bowel cancer is very low. The most common symptoms are abdominal pain, nausea, vomiting, and overt gastrointestinal tract bleeding. The most frequent endoscopic findings of small bowel cancer are stenosis or ulceration, followed by submucosal tumors and multiple white nodules.4 In addition, the most frequent location for small bowel tumors is the jejunum, followed by the ileum and duodenum.2
Although there are some differences between the studies reported to date, the most common metastatic cancers involving the small bowel are primary tumors such as malignant melanoma, colon cancer, cervical cancer, and ovarian cancer.7 Metastasis to the small bowel is usually hematogenous or due to direct invasion from intraperitoneal seeding. Primary cancers of the colon, ovary, uterus, and stomach are usually spread to the small bowel by direct invasion or intraperitoneal spread, whereas primary cancers from the breast, lung, and melanoma metastasize to the small bowel by a hematogenous route.8 The overall incidence of metastatic small bowel cancer is very low, and as mentioned earlier, most metastatic cancers have neither specific symptoms nor signs until they cause small bowel obstruction. Therefore, it is very difficult to detect metastatic small bowel cancer. Due to the delays in diagnosis, patients with metastatic small bowel cancer are diagnosed at relatively advanced stages and usually have a poor prognosis.4
The present case involved small bowel obstructions of unknown origin in a patient with a history of multiple cancers. Patients with small bowel obstruction usually require surgical resection to relieve the obstructive symptoms and diagnose the etiology. However, the preoperative assessment of small bowel obstructions by DBE enables surgeons to perform a scheduled operation by confirming the preoperative pathologic findings of the cancer's etiology, and to prevent extensive small bowel resection by determining the extent or location of obstructive lesions. Moreover, in recent years, the role of BAE has expanded. Besides diagnostic evaluation, deep small bowel enteroscopy enables the widening of bowel-obstructive lesions by endoscopic guided metal stent insertion.9
Recurrence or metastasis of breast cancer is common, and occurs in 20%-30% of patients. The common sites for breast cancer metastasis are bone, lung, liver, and brain.7,10 Metastasis to the gastrointestinal tract is uncommon and when it does occur, it mainly involves the stomach, colon, or rectum.11,12 Metastasis to the small bowel is very rare, comprising approximately 0.08% of metastatic breast cancers.13 There are very few reports of the small intestinal metastasis of breast cancer.
In the present case, metastatic small bowel cancer was diagnosed 6 years after the initial diagnosis of breast cancer. The median interval for recurrence after surgical resection for breast cancer is 2 to 3 years, and recurrence is within 5 years in 90% of cases, although a 30-year interval between the initial diagnosis of breast cancer and the presentation of metastasis has been reported in the literature.7,11 Therefore, metastatic small bowel cancer should be considered in patients with gastrointestinal symptoms or a newly identified gastrointestinal neoplasm, especially those with a history of colon cancer, ovarian cancer, lung cancer, or breast cancer, even if the patients were diagnosed with cancer a long time ago.14
In this paper, we reported small bowel obstruction due to small bowel metastasis from breast cancer diagnosed by DBE in a patient with a history of multiple cancers. To our knowledge, this is the first detailed report of the preoperative diagnosis of small intestinal metastatic breast cancer by DBE. Small bowel metastatic cancer is a rare disease and not easy to detect early. There is no doubt that DBE is one of the most useful devices for approaching a suspected small bowel tumor, and for making a histological diagnosis before surgery.