INTRODUCTION
Endoscopic submucosal dissection (ESD) is an innovative endoscopic technique that allows for en bloc resection of superficial gastrointestinal tumors regardless of their size. This allows for the precise histopathological assessment of specimen margins and reduces the risk of recurrence compared with endoscopic piecemeal mucosal resection (EPMR) on long-term follow-up.1,2,3 In Korea and Japan, ESD is routinely performed in the endoscopic treatment of superficial gastric neoplasias,4,5,6 and is becoming the standard treatment for colorectal neoplasias such as early colorectal cancer or benign colorectal tumors ≥2 cm for which en bloc resection with conventional endoscopic mucosal resection (EMR) is difficult. In a comparative study of ESD versus EMR for colorectal tumors ≥2 cm,7,8,9 there was a 2% recurrence rate in the ESD group versus 14% in the EMR group, which also required additional EMR.
However, there are some limitations in performing colorectal ESD, as colorectal ESD is technically more difficult than conventional EMR and has a high risk of complications such as perforation and bleeding. Furthermore, serious peritonitis can develop from colonic perforation and as a result of secondary contamination by colonic bacteria and feces.5,7,10 Therefore, accurate preprocedural diagnosis of the lesion and selection of the appropriate treatment from a precise diagnosis are important. According to a recent guideline,11 when endoscopic treatment is performed for a large colorectal tumor, en bloc resection such as ESD is the principal approach. However, piecemeal resection is also acceptable except in cases of definitive submucosal invasion. In addition, depending on the skill of the endoscopist or the current practice in the hospital, there can be variations in the selection of the treatment method.
Colorectal ESD was introduced in Korea in 2003 and is now being routinely performed at major teaching hospitals. The outcomes of colorectal ESD in Korea are comparable to those in Japan.4,12 However, the indications for colorectal ESD are still controversial. To establish colorectal ESD as a standard treatment, consistent preprocedural diagnosis of the colorectal lesion and selection of appropriate treatment options are required. In order to establish a standard indication for colorectal ESD, we sought to investigate the preferred criteria of ESD experts for colorectal ESD in their practice.
METHODS
1. Study Subjects and Methods
Multiple-choice questionnaires were sent to 27 expert members of the Korean Society of Gastrointestinal Endoscopy/ESD group and the Korean Association for the Study of Intestinal Disease. The potential participants were gastroenterologists experienced in colorectal ESD at tertiary referral centers. In June 2013, they were asked to complete the questionnaire via e-mail. Of the 27 gastroenterologists, 18 completed the survey (response rate, 66.7%). Among these, nine had performed colorectal ESD in >100 cases, and the remaining had performed the procedure in <100 cases.
The survey consisted of 33 questions that explored the criteria for selecting a treatment method for colorectal tumors (Table 1). In this study, we defined shallow submucosal invasion as <1,000 µm and massive submucosal invasion as >1,000 µm. In selecting a therapeutic approach, assessment of clinicopathologic characteristics of the tumor is important, and several factors or situations must be taken into consideration. These include (1) preprocedural histology, (2) endoscopic gross morphology of the tumor, (3) presence of a depression or ulcer on the surface of the tumor, (4) the pit pattern of the tumor (by Kudo classification),13 (5) narrow band imaging (NBI) pattern of the tumor (by Sano-Emura classification),14 (6) lifting or nonlifting sign of the tumor, (7) sporadic localized tumor in chronic inflammation, and (8) local residual early cancer after endoscopic resection. For each situation, the survey asked, “which method was the optimal treatment option?” (1) EPMR (or preferring EPMR), (2) either EPMR or ESD, (3) ESD (or preferring ESD), (4) either ESD or surgery, and (5) surgery (or preferring surgery). The 18 participants decided on their most appropriate treatment method in five options. The survey was completed anonymously. Moreover, there were no costs or patient contact involved, and the survey carried no risks. As we did not use patient information, Institutional Review Board approval was not required.
RESULTS
The results consisted of 33 questions and answers that explored the indications of endoscopists for selecting a treatment method in colorectal tumors ≥2 cm (Figs 1,2,3,4,5,6). The colorectal ESD indication for colorectal tumors <2 cm is also presented in Supplementary Fig. 1.
1. Decision Making Based on the Preprocedural Assessment of Histology for the Treatment of Tumors ≥2 cm in Diameter
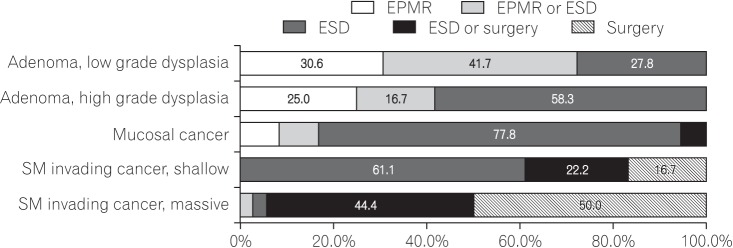
Fig. 1 presents the results of questions that addressed the decision of endoscopists concerning the treatment method based on the preprocedural histologic assessment of the tumor. When the preprocedural histologic diagnosis was low-grade adenoma, 41.7% of endoscopists selected EPMR or ESD, and another 30.6% selected EPMR for the treatment of the tumor. For high-grade adenoma, 58.3% of endoscopists selected ESD and another 25.0% selected EPMR for the treatment of the tumor. For mucosal cancer, 77.8% of endoscopists selected ESD. For shallow submucosa invasive cancer, 61.1% of endoscopists selected ESD and another 22.2% selected surgery or ESD for the treatment of the tumor.
2. Decision Making Based on Endoscopic Gross Morphology for the Treatment of Laterally Spreading Tumors ≥2 cm in Diameter
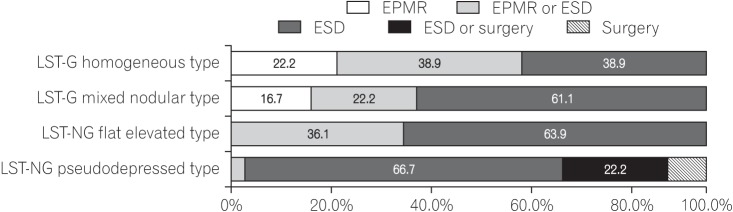
Fig. 2 presents the results of questions that addressed the decision of endoscopists about the treatment method based on the endoscopic gross morphology type of laterally spreading tumors (LSTs). When the gross morphology of the tumor is LST-granular (LST-G) homogeneous type, 38.9% of endoscopists selected EPMR or ESD. For LST-G nodular mixed type, 61.1% of endoscopists selected ESD and another 22.2% selected EPMR. For LST-nongranular (LST-NG) flat elevated type, 63.9% of endoscopists selected ESD and another 36.1% selected EPMR or ESD. For LST-NG pseudodepressed type, 66.7% of the endoscopists selected ESD and another 22.2% selected surgery or ESD.
3. Decision Making Based on the Pit Pattern (Kudo Classification) for the Treatment of Tumors ≥2 cm in Diameter
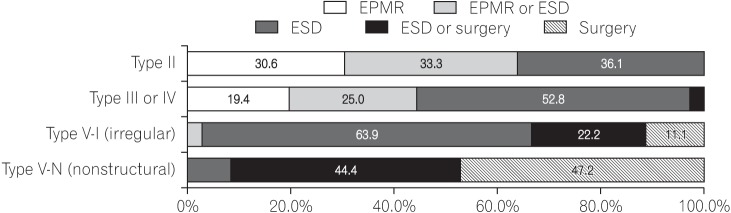
Fig. 3 presents the results from questions that addressed the decision of endoscopists about the treatment method based on the pit pattern of the tumor. When the tumor showed a type II pit pattern, 36.1% of endoscopists selected ESD and another 33.3% selected EPMR or ESD for the treatment of the tumor. For tumors with type III or IV pit pattern, 52.8% of endoscopists selected ESD and another 25.0% selected EPMR or ESD. For tumors with type V-I (irregular) pit pattern, 63.9% of endoscopists selected ESD and another 22.2% selected surgery or ESD. For tumors showing type V-N (nonstructural) pit pattern, 47.2% of endoscopists selected surgery and another 44.4% selected surgery or ESD for the treatment of the tumor.
4. Decision Making Based on the NBI Pattern (Sano-Emura Classification) for the Treatment of Tumors ≥2 cm in Diameter
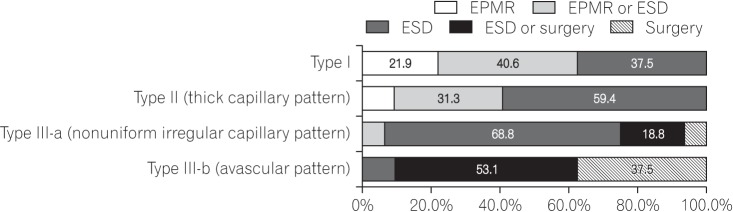
Fig. 4 presents the results from the decision of endoscopists about the treatment method based on the NBI pattern of the tumor. When the tumor showed type I NBI pattern, 40.6% of endoscopists selected EPMR or ESD and another 37.5% selected ESD. For tumors with type II (thick capillary) NBI pattern, 59.4% of endoscopists selected ESD and another 31.3% selected EPMR or ESD. For tumors showing type III-a (nonuniform irregular capillary) NBI pattern, 68.8% of endoscopists selected ESD. For tumors showing type III-b (avascular) NBI pattern, most of the endoscopists (53.1%) selected surgery or ESD and another 37.5% selected surgery for the treatment of the tumor.
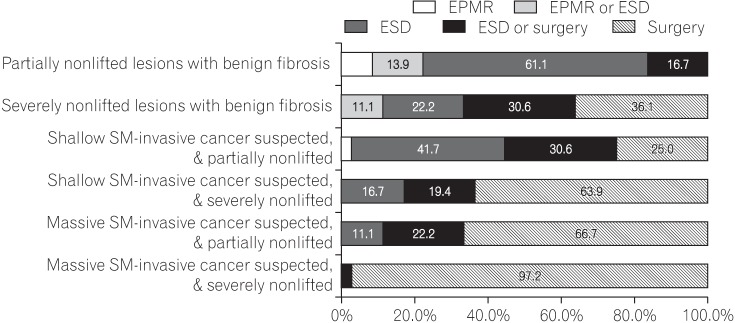
5. Decision Making Based on the Nonlifting Sign for the Treatment of Tumors ≥2 cm in Diameter
Fig. 5 presents the results from the decision of endoscopists about the treatment method based on the nonlifting sign of the tumor. When the tumor showed a partially nonlifting sign with benign fibrosis, 61.1% of endoscopists selected ESD. For tumors showing severe nonlifting sign with benign fibrosis, 36.1% of endoscopists selected surgery and another 30.6% selected ESD or surgery. For tumors that showed a partially nonlifting sign and suspected shallow submucosa-invasive cancer, 41.7% of endoscopists selected ESD and another 30.6% selected ESD or surgery. For tumors that showed severe nonlifting sign and suspected shallow submucosa-invasive cancer, 63.9% of endoscopists selected surgery and another 22.2% selected ESD or surgery for the treatment of the tumor.
6. Decision Making Based on the Presence of Depression or Ulcer on the Surface of Tumors ≥2 cm in Diameter
Fig. 6 presents the results from questions that addressed the decisions of endoscopists about the treatment method based on the presence of a depression or ulcer on the surface of the tumor. For any tumor with a depressed area, 58.3% selected ESD and another 33.3% selected surgery or ESD. For any tumor with an ulcer, 47.2% of endoscopists selected surgery and another 30.6% selected ESD or surgery.
7. Decision Making in Special Situations Such as Sporadic Localized Tumors in Chronic Inflammation and Local Residual Early Cancer after Endoscopic Resection
Fig. 6 presents the results from questions that addressed the decision of endoscopists about the treatment method in special situations. For sporadic localized tumors in chronic inflammation, 52.8% of endoscopists selected ESD and another 22.2% selected EPMR or ESD. For local residual early cancer after endoscopic resection, 38.9% of endoscopists selected ESD and another 36.1% selected surgery for the treatment of the tumor.
8. Preference for Evaluation Tools for Depth of Tumor Invasion
Table 2 presents the results from questions that addressed the preference of endoscopists about the tool for evaluating the depth of tumor invasion. Korean endoscopists rarely (<10%) or sometimes (10%-50%) use EUS for decisions about colorectal ESD. NBI is used sometimes (10%-50%) in selecting ESD for colorectal neoplasms. Magnification endoscopy is used rarely (<10%) in selecting ESD for colorectal neoplasms. In practice, endoscopists most commonly use gross morphology patterns such as size, shape, and surface to determine the treatment modality for colorectal neoplasms. Korean endoscopists believe that magnifying endoscopy and EUS are the most accurate methods for evaluating the depth of tumor invasion; however, they do not believe that either magnifying endoscopy or EUS are practical, usable options.
DISCUSSION
With the development of various endoscopic tools, devices, increased experience, and growing expertise in ESD, colorectal ESD is now routinely performed in Korea. Originally used for gastric tumors and not for colorectal tumors, there are, however, important differences between superficial gastric tumors and superficial colorectal tumors. These include gastric tumors usually being carcinomatous, whereas colorectal tumors are mostly benign lesions.6,15 The rate of local recurrence after piecemeal resection of intramucosal tumors of the colorectum has increased;10,16 however, even in such cases, residual or recurrent tumors can be treated with repeated endoscopic resection or surgery. In this regard, en bloc resection of colorectal tumors is less absolute than that of gastric tumors. At the same time, the advances in magnifying endoscopy with dye-spraying and image-enhancement endoscopy have enabled the preprocedural assessment of histology and invasion depth of tumors with high accuracy.17,18,19
In this study, we surveyed the criteria of endoscopists for indicating colorectal ESD in their practice. From the survey, lesions such as LST-NG or tumors with type V-I pit pattern or type III-a NBI pattern, or tumors with a depressed area or shallow submucosa-invasive cancer cases were favored for colorectal ESD. These lesions have a significantly higher possibility of submucosal invasion and require en bloc resection for an accurate pathological evaluation. Other types of lesions chosen for colorectal ESD include tumors with partial submucosal fibrosis, tumors with partially nonlifting shallow submucosal invasion, tumors that are sporadically localized in the background of chronic inflammation, and cases of local residual early cancer after endoscopic resection. These types of lesions are included in the indication for ESD because the lesions are technically difficult to treat with conventional EMR. The selection criteria for colorectal ESD from our survey are almost the same as the indications for colorectal ESD in Japan.11 In addition, more benign-looking tumors tended to be included in clinical practice for colorectal ESD, as LST-G nodular mixed type, tumors with types III and IV pit pattern, and serrated tumors with type II NBI pattern are mostly benign lesions confined to the mucosa. In practice, the indications by Korean endoscopists for colorectal ESD are broader than those in the recent guidelines.11,20
Comparisons of outcomes for colorectal ESD versus EMR for large colorectal tumors have been reported in several clinical studies.10,21,22 For large colorectal tumors, ESD had higher en bloc resection rates and lower recurrence rates than EMR, but had higher complication rates and required a longer procedure time. Although the local recurrence rates of the EMR group were higher than those of the ESD group, 89.8% of recurrent cases were successfully treated with additional EMR. Only 10.2% of recurrent cases required additional surgical resection.10,22 Therefore, EPMR for large colorectal tumors is an acceptable treatment method. Significantly, when preprocedural diagnosis is performed precisely, recurrent lesions will usually be adenomas and additional endoscopic resection will be successful without surgical treatment.
Before performing colorectal ESD or EMR, diagnosis based on image-enhanced endoscopy and magnifying endoscopy allows for the distinction of a carcinoma from an adenoma and for estimating the invasion depth of the tumor.23,24 The diagnostic accuracy rate of discrimination between adenoma and carcinoma was 70% to 90% for pit pattern diagnosis with magnifying observation, and a similar rate was obtained by using image-enhancement endoscopy such as NBI.17,18,19 There are two subtypes of LST, namely LST-G and LST-NG. The rate of submucosal invasion in LST-NG was significantly higher than that of LST-G. In LST-G nodular mixed type, submucosal invasion may exist in a large nodule or an area of a type V-I pit pattern.25 Importantly, EPMR without breaking the carcinomatous portion into fragments should be applied. For LST-NG cases, the lesion should be removed en bloc with ESD because there is a higher potential for invasion and fibrosis, and the specimen obtained from the complete en bloc excision can be pathologically evaluated in detail.20,25,26,27
From our survey, endoscopists tend to conduct colorectal ESD for apparent adenomatous LST lesions in their practice. Although en block resection such as ESD is desirable if applicable, colorectal ESD is technically difficult, time consuming, and has a high risk of complications such as perforation. The objective of endoscopic treatment for adenoma is elimination of the lesion; therefore, EPMR is a good alternative treatment method for eliminating an obvious adenoma. Through precise preprocedural diagnosis, prearranged EPMR with minimal fractions is an appropriate treatment method for adenomatous LST lesions. Endoscopists should not perform superfluous ESD merely to improve their own ESD skills or for other reasons of self-interest, as this could unnecessarily place the patient at a risk of complications. To establish a standard indication for colorectal ESD, it is important to balance the need for completeness of treatment versus patient safety and simplified treatment.