Dear sir,
It was with great interest that we read the article entitled "Clinical and Endoscopic Recurrence after Surgical Resection in Patients with Crohn's Disease", recently published in this journal by Yang Woon Lee and colleagues.1 The article describes one of the first retrospective experiences with Korean patients regarding the rates of both clinical and endoscopic recurrence (ER) after surgical abdominal procedures for CD. In this study, the authors found an overall rate of ER of 71.4% (15 from 21) patients, in a mean follow-up period of 50.5 months.
Although the study adds very important real world data and represents one of the first experiences on the topic of ER in Korean patients, some considerations are important in this data analysis and must be taken into consideration.
First, the population of the study is somehow heterogeneous. A myriad of operations was performed as they fulfilled the inclusion criteria. Most of the western studies were performed only after ileocecal resections,2,3 and in this interesting Korean retrospective study, small bowel resections, segmental colectomies and other different procedures were also included. The Rutgeerts's score is not fully validated after different procedures, it is mostly widely used after ileocecal resections, and there is significant controversy if it can be applied after other operations, even with capsule endoscopy to detect recurrence.4 Moreover, most of the western studies consider the definition of ER as a Rutgeerts' score Ōēźi-2, considering the i-1 score as mucosal normality, differently of the criteria of the Korean study.1,2,3,4 However, only one patient in the sample presented as an i-1 after surgery, what would not influence significantly the final results of recurrence.
There is quite a consensus in the literature that smoking, previous resections and penetrating CD are significant risk factors for ER in CD patients.3,5 The study did not find any risk factor, despite meticulous statistical analysis, maybe for 2 reasons: the small number of patients in the sample, or the possibility of a different genetic background in Korean CD patients, that can alter the phenotype of the disease in the country, as previously stated by the authors.
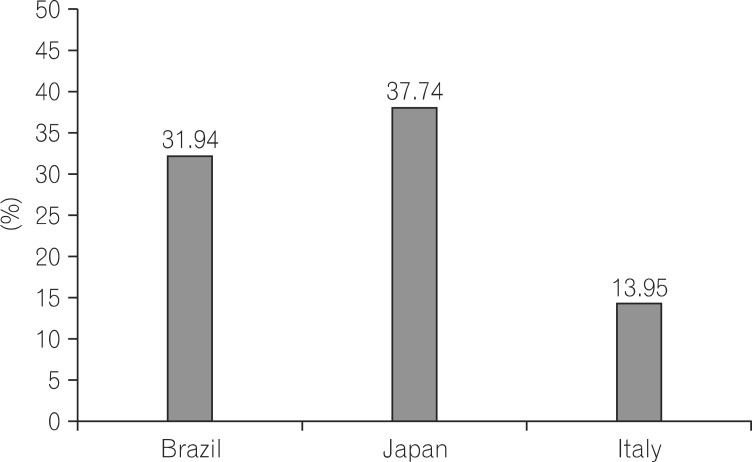
We recently presented at the European Crohn's and Colitis Organisation (ECCO) congress the results from a database with patients from 7 referral centers from South America, Europe and Asia regarding the same topic as this interesting Korean study.6 In our experience, ER was observed in aproximately 32% of patients treated in Brazil, 38% of those treated in Japan and in 14% of patients treated in Italy (Fig. 1). These lower numbers, as compared to the Korean study, probably were observed due to the shorter follow-up period of 12 months in this database. However, they could also be a consequence of a similar strategy of postoperative prevention of recurrence that is actively practised in these referral centers.6 The differences between the Korean study as compared to ours, are also basically related to the different populations analyzed.
Despite these few considerations, we would like to congratulate the staff from the Catholic University of Korea for this new interesting information on ER after CD surgical procedures in Asian patients. We also hope that this data can impact in a near future in the prospective management of surgically-treated CD patients in Korea, increasing the number of colonoscopies or other endoscopic examinations performed 6 to 12 months after surgery, in order to detect early ER, optimize medical therapy if needed, and possibly to lead to a lower rate of recurrence in the long term and better control of the disease.