INTRODUCTION
Incidence rate of IBD is stabilizing in some developed countries [1-4]; however, the incidence rate is increasing in developing countries such as Asia and Eastern Europe [5-7]. Recent nation-wide report in Iran showed the increasing trend in incidence and prevalence of both UC and CD [8]. The rising incidence and prevalence of IBD made an essence to investigate the risk factors and possible etiologies of this disease and necessitates further studies for better understanding of natural history, phenotype, treatment response, complication, and survival of the patients who suffer from IBD. Establishing a prospective IBD registry is one the best way to answer these questions [9].
Iranian ministry of health have recently launched a program of supporting disease registries [10]. Following this initiative, we established a multicenter national IBD registry named “Iranian Registry of Crohn’s and Colitis (IRCC).” Each disease registry has its own limitation and strength and thereby could not answer all clinical or epidemiological questions related to that disease [11]. Introducing the study design, data collection, and aims of IRCC enlighten the strengths and limitations and may help researchers to better interpret the results of this nation-wide study in future.
The aim of IRCC is to study clinical phenotype, safety of treatment, pattern of care across country, risk of colorectal cancer, prognostic factors, complication, survival, incidence and prevalence of IBD in Iran. Another objective is to set up a blood and stool biobank of IBD patients which its protocol will be published in near future. In this report we described the study protocol, process of IRCC implementation and assessment of its feasibility in Iran.
METHODS
1. Registry Setting and Organization
IRCC is a multicenter prospective registry enrolling adult patients diagnosed as IBD. Patients are managed according to their routine care and no intervention from the registry team would be imposed. The registry comprises of referral centers of IBD located in the capital and all provincial centers of Iran.
IRCC was organized under the guidance of steering committee of 7 senior gastroenterologists from major gastroenterology departments and research centers of Iran. These members were selected based on their expertise and interest in research and care of IBD patients. One member of steering committee was selected as principal investigator and director of registry in order to supervise the executive team (Fig. 1) which consists of an executive manager, 2 registrars, a nurse as patient educator, an information technology (IT) technician and 2 researchers. Gastroenterologists who shared their cases with registry were considered as IRCC collaborators. The executive team had a time chart and objectives for each year which were followed in weekly regular meeting. An authorship guideline was approved by steering committee after receiving comments from all collaborators. The study was approved in Ethic Committee of Digestive Disease Research Institute of Tehran University of Medical Sciences. IRCC was funded by deputy of research of the Ministry of Health and Medical Education and was strongly supported for all logistics by the Iranian Association of Gastroenterology and Hepatology (IAGH).
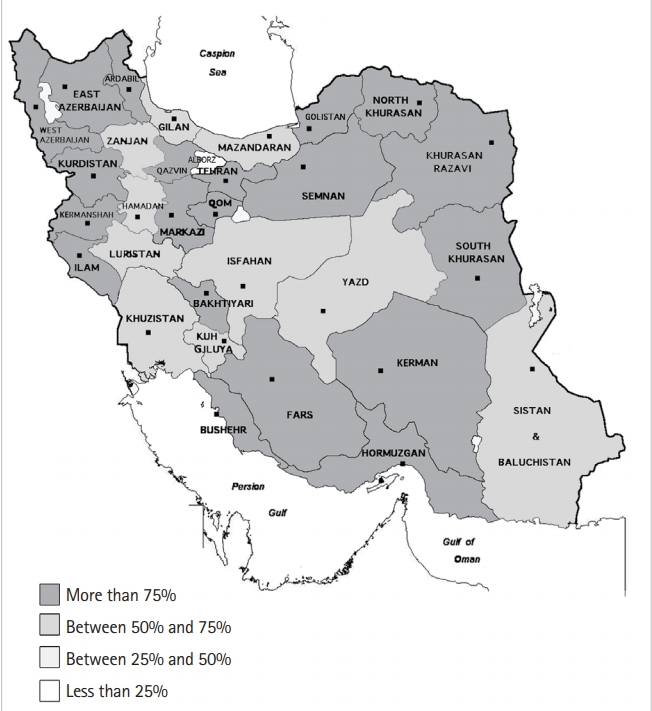
In Iran, all IBD patients were served at provincial center rather than villages or small cities. IRCC has at least 1 center in each province. From different provinces, 449 gastroenterologists who visit IBD patients in public or private clinics have accepted to collaborate with IRCC. According to report from IAGH 517 gastroenterologists are presently working in Iran. Therefore, IRCC covers 87% of all GI centers around the country (Fig. 2, Supplementary Table 1). However, the exact participation rate could be calculated after finishing the registry process. Of different provinces of Iran, the most modernized and industrialized are Tehran, Razavi Khorasan, Fars, Isfahan, Mazandaran, East Azerbaijan, and Gilan in which the majority of gastroenterologists work and most of IBD patient were treated there. Distribution of gastroenterologists in Iran was shown in Supplementary Table 1 and Supplementary Fig. 1.
2. Study Population
Study population consisted of adult who were diagnosed as IBD by gastroenterologists in collaborating centers across the country. The exclusion criteria were set for patients who aged less than 18 years and for those who were unable or unwilling to provide informed consent. Patients with un-confirmed diagnosis also were excluded.
3. Disease Definition
IBD is defined as combination of clinical, radiological, colonoscopic, and pathologic and classified to UC and CD according to international IBD guideline [12] as below. This uniform criterion was attached as appendix to IRCC questionnaire and sent to all collaborating provincial centers.
1) Clinical
History of rectal bleeding or bloody mucus diarrhea, abdominal pain, vomiting, weight loss, fistulas, and fever. Finding such as pallor, cachexia, mild abdominal tenderness, perianal involvement (fissure, fistula, and abscess) in physical examination. Predominantly bloody diarrhea was in favor of UC. Abdominal pain, malnutrition, and perianal lesions were in favor of CD.
2) Laboratory Tests
Evidence of anemia and thrombocytosis in complete blood count, elevated ESR or CRP, negative stool exam and culture to rule out bacterial or parasitic infection and elevated level of fecal calprotectin. Anti-neutrophil cytoplasmic antibody and Anti-Saccharomyces cerevisiae antibody were in favor of UC and CD respectively.
3) Colonoscopic
Evidence of ulcers, aphthous lesions, inflammation, bleeding, stenosis, pseudo-polyps in colon. Capsule endoscopy and enteroscopy were used in cases of small bowel involvement when other modalities have been negative and IBD was strongly suspected. Continuous superficial colonic mucosal lesions, and spontaneous bleeding were in favor of UC. Patchy transmural asymmetric lesions mainly involving ileum and right-sided colon, deep fissures, cobblestone appearance, and longitudinal ulcers were in favor of CD.
4. Disease Activity
Disease activity were assessed by international patient-centered instruments which were mostly based on clinical symptoms and were validated and correlated with colonoscopic, laboratory, and imaging findings. IBD-control-8 questionnaire for checking patients’ recent symptoms (score more than 13 indicates inactive disease) [13] and Manitoba IBD index for checking disease control in 6 months before interview (score more than 4 indicates inactive disease) were used in IRCC questionnaire [14].
5. Drug Availability
More than 95% of Iranians are covered by national health insurance and cost of almost all IBD-related drugs including biologics are supported. Furthermore, patients have access to all type of treatments including anti-TNF drugs. Therefore, the pattern of IBD treatment in Iran would not be affected by drug availability.
6. Questionnaire
We define our minimum data set for IRCC according to an international consensus on standard set of patient-centered outcome for IBD which has been reported recently [15]. The questionnaire has been developed and agreed following an exhaustive consultation process with technical supervisors and steering committee. And contains following sections: demographics, habitual, comorbidities, disease activity, quality of life, healthcare utilization, treatment complications, survival and disease control (Table 1, Supplementary Material 1). Standard queries were included in the questionnaire to interview patients on education level [16], past medical history [17], symptoms of IBD in last 2 weeks [13] and disease control in last 6 months [14]. Questions containing information on disease subtype, extent of intestinal involvement, clinical phenotype, and IBD-related surgery were specified to be answered by physician (clinician-reported). Since opium and hookah use is common in Iran, related questions were added to questionnaire in order to evaluate their association with IBD.
7. Enrollment
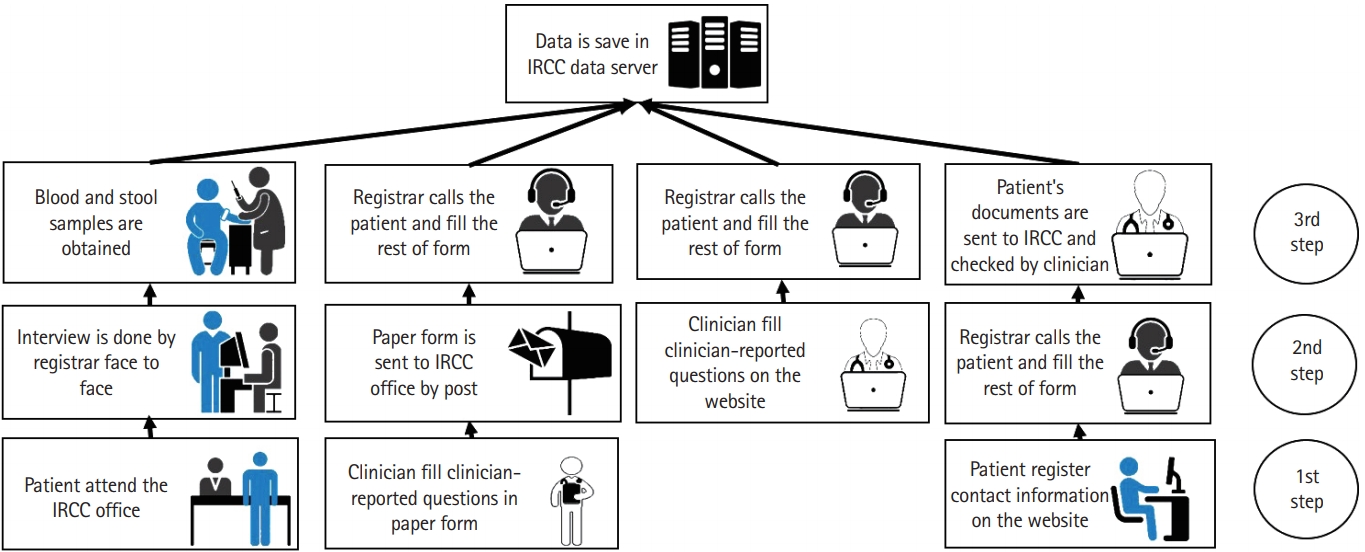
In order to enroll cases, a web-based software and website [18] were designed by our IT technician. Collection of data would be performed in different ways after obtaining the consent from patients (Fig. 3). Any gastroenterologist could register his/her IBD patient information in the web-based software primarily and then the registrar from IRCC office calls the patient and fills the rest of questions. Patient enters his/her contact information directly into the web-based software. Registrar then calls the patient and fills the rest of questions. Any IRCC collaborator could fill a paper-based questionnaire and then sends it to the IRCC office by post to be entered to the database by registrars. Patient can directly refer to IRCC office and provides the necessary information to the registrar. For confidentiality of data, our software generates an identification code for each case which would be used for exporting anonymized data.
8. Follow-up
After enrolling IBD patients, annual telephone call will be made to each patient and data about treatment complications, symptoms and quality of life, admission and emergency department visits, and disease control will be collected. In addition, all IRCC collaborators are available to help and complete the follow up data. Any outcome such as, IBD flare-up, IBD-related surgery and disability and death will be recorded and related documents will be reviewed accordingly.
9. Pilot Study
To evaluate the feasibility of our project, we designed a pilot study on 553 IBD patients whom their contact information was available. The majority of studied subjects (n=529, 95%) were registered primarily by their gastroenterologist with paper-based questionnaire and then the registrar from IRCC office called them for interview. The minority of patients (n=12, 2%) attended the IRCC office directly and 17 patients (3%) were registered into the website by their physician. At the end of pilot study, all IRCC collaborators were invited and the study design, data collection, questionnaire and results of pilot study were presented. All comments on study protocol were considered and the final version of questionnaire was developed. The quality control protocol for process of data collection and data accuracy was defined according to the caveats in pilot study.
10. Quality Control of Registry Process
Case enrollment was based on diagnosis of IRCC collaborators who were committed to use standard disease definition and protocol. Quality of data collection was monitored by random recording and checking of interviews performed by registrars. Moreover, our designed software has some validation rules which does not let wrong data to be registered and it has monitoring dashboard for executive manager to follow rate of response and missing data. All registrars were trained in the IRCC office.
11. Quality Control of Data
We used standard minimum data set of outcomes related to IBD [15], to guarantee that our data would be comparable to other IBD registries throughout the world. As IRCC collaborators were committed to share the information of eligible cases, we can assume that selection bias is minimal. We expect the completeness of collected data by using the IRCC software which has obligatory fields for necessary questions. There is also a protocol for random checking of questions answered by physician in order to check the construct validity of clinician-reported questions. Annual report will be released and sent to registry office at deputy of research in ministry of health and all IRCC collaborators.
12. Statistics
Face validity of our questionnaire was checked by multiple sessions of expert panel for reviewing the questions and by receiving feedbacks from registrars during and after pilot study. The reliability of each section was evaluated by Cronbach’s α. We used chi-square test for comparing categorical variables and ANOVA with Bonferroni post hoc test for comparing continuous variables. P-value less than 0.05 considered significant. Analysis carried out using STATA software, version 11 (StataCorp LLC, College Station, TX, USA).
RESULTS
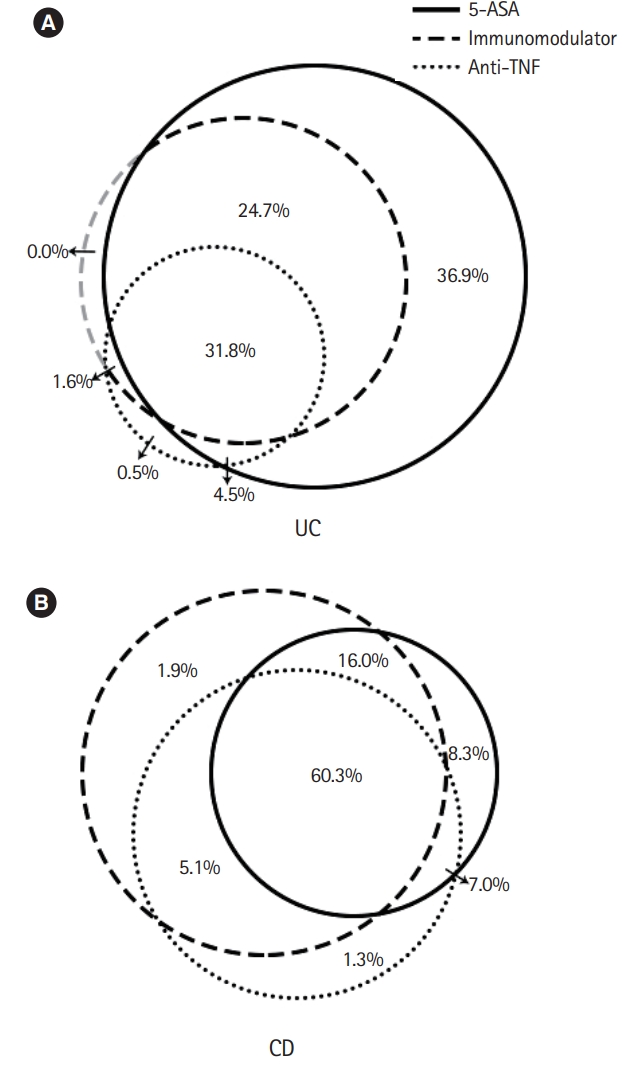
The mean age of participants was 38.60 years (SD, 12.86) with 312 of them were male (56.42%). About half of subjects (n=303, 54.78%) had university education. Fars ethnicity comprise 64.74% of our enrolled subjects (n=358). Majority of registered subjects had UC (n=378, 68.35%). We observed that 68 of patients (12.30%) were smoker and 44 subjects (7.96%) were hookah users and only 13 patients (2.35%) reported opium consumption. Fifty-eight patients (10.48%) had history of appendectomy of which 30 cases were before diagnosis of IBD. Family history were positive in 65 subjects (11.75%) for first degree (50 relatives had UC) and 38 (6.87%) for second-degree relatives (29 relatives had UC). The age at diagnosis for UC and CD were 31.36 (SD, 12.16) and 27.92 (SD, 11.32) years respectively (P=0.00). Disease duration were similar in both subgroups of UC and CD (8.40±7.26 and 8.18±7.18 years, P=0.91). Most of patients (n=341, 61.66%) had quiescent disease in 2 weeks before enrollment and 289 patients (52.22%) had IBD in remission during the last 6 months (Table 2). 5-Aminosalicylate (5-ASA) and immunomodulator (azathioprine or 6-mercaptopurine or methotrexate) were currently used by 67.81% and 43.58% of participants, respectively (Table 3, Fig. 4). The reliability of each section of questionnaire was checked and all sections had Cronbach’s α>0.6 (Table 4).
Compared to patients with UC, those with CD were treated more frequently with immunomodulator (azathioprine or 6- mercaptopurine or methotrexate) (38.36% vs. 70.99%, P<0.001) or anti-TNF (adalimumab or infliximab) (57.94% vs. 80.25%, P<0.001). There was no significant difference in disease activity score between patients whom were treated with adalimumab compared to those consumed infliximab (P=0.52).
DISCUSSION
In this paper, we introduced the design and implementation of IBD registry in Iran named “IRCC.” Although there were few IBD registries at provincial level in Iran [19,20], to best of our knowledge, this is the first nation-wide registry running in Middle East. We have assessed the feasibility of our study and face validity and internal reliability of designed questionnaire by performing a pilot study on 553 subjects.
Although registry is a prospective observational study and patients are not randomly assigned to specific treatment, its result is as powerful as randomized controlled trials (RCT) or cohort studies, because patients are followed in their real-world life and are not excluded due to different study criteria. Moreover, the follow-up duration is always longer than RCTs. These advantages could help investigators to more efficiently evaluate the natural course of disease and obtain more accurate date regarding treatment response and disease survival [21].
Similar to IRCC, multicenter registries are held in other part of the world. For example, SHARE registry in the United States is cooperation of 7 referral IBD centers focused mostly on biomedical researches and treatment of IBD [22]. There are also multicenter IBD registries in Europe such as Austrian IBD center cohort which is comprised of 14 tertiary centers and aimed to study on disease phenotype and activity and treatment of IBD [23]. In Asia, there are 2 multihospital registries held in china and 1 in Hong Kong which epidemiologic data from these registries were reported [24-26]. Also there is an ongoing multicenter nation-wide IBD registry in Korea [27]. Although IRCC is a multicenter IBD registry at present time, but we have planned to expand it by including all GI centers around the country. This task is more achievable with establishment of ongoing electronic medical record system in Iran. Because we would be able to use these records by IRCC software similar to other registries such as IBD UK registry [28] or IBD registry at Western Pennsylvania [29].
Another very important initiative is the International Inflammatory Bowel Disease Genetics Consortium which is a network of world researchers focusing mainly on the genetics of IBD. It has undertaken a number of large-scale genome-wide association studies of CD and UC, and have been able to identified more than 200 IBD risk loci with majority of these loci are shared across diverse ancestry groups, including Iranian [30]. By setting up bio-bank of IBD patient in Iran further studies on IBD genetics will be possible. Also collecting blood samples will be useful for study on new biomarkers for diagnosis and monitoring IBD and colleting stool samples will help to study the role of microbiota in IBD etiology and disease activity.
There are several strengths in this study including a prospective design, using a validated and reliable questionnaire based on accepted international minimum data set [15], a well-designed software and website, flexible options to enroll IBD cases, and registering patients with their unique national ID which will allow data linkage to other national studies such as cancer registry and cause of death registry. There are also some limitations such as absence of link to patients’ detail medical records at present time and before establishment of national electrical medical record in Iran.
In conclusion IRCC could become a reliable infrastructure for national and international research on IBD and at the same time improve the care of IBD patients and provide national information for policy makers to better plan for controlling IBD in Iran.