INTRODUCTION
The number of patients with inflammatory bowel disease (IBD) in Asia is increasing annually [1,2]. Asia will therefore be important toward advancing the global IBD field. Asian and Western IBD patients differ in both their genetic backgrounds and several clinical features [2,3]. As such, clinical trials for newly developed drugs should confirm the efficacy and safety in both Asian and Western patients [4-6].
CrohnŌĆÖs disease (CD) is a progressive disease, but patient prognosis can be improved using a treat-to-target strategy with continuous scheduled objective monitoring [7,8]. In contrast to ulcerative colitis, the gastrointestinal lesions of CD can occur anywhere from the mouth to the anus. Therefore, it is important to assess the existence, activity, and complications in a broad area compared over long-term periods in clinical management. The small bowel (SB) is an especially common location for CD lesions, making objective monitoring more difficult for CD lesions than for colonic lesions.
Tight control of SB lesions is a key factor in the clinical management of CD. Therefore, the strategies and techniques for diagnosing, monitoring, and treating SB lesions in patients with CD must be optimized [9].
IMPORTANCE OF SB LESIONS IN PATIENTS WITH CD FOR CLINICAL PRACTICE
Why are SB lesions in patients with CD important in clinical practice? de Barros et al. [10] demonstrated the importance of the location of SB lesions according to the Montreal classification with a 65.2-month follow-up. An ileal (L1) lesion was more significantly associated with a complicated disease course (relative risk [RR], 1.64; 95% confidence interval [CI], 1.10-1.75) and stricturing behavior (RR, 2.11; 95% CI, 1.20-3.69) than a colonic (L2) lesion. Further, L1 lesions are also associated with poorer abdominal surgery outcomes compared to ileocolonic (L3) lesions (RR, 1.68; 95% CI, 1.13-2.50). In another investigation using data obtained from the REACT trial involving 1,898 CD patients, SB lesions were more strongly associated with CD-related surgery than colonic lesions (odds ratio [OR], 2.03; 95% CI, 1.16-3.57) [11]. At our institute, SB lesions are the lesions most frequently responsible for surgery in patients with CD [12]. It is critical to recognize the importance of SB lesions in the clinical management of patients with CD.
FEATURES OF SB LESIONS IN PATIENTS WITH CD
ŌĆ£Silent CDŌĆØ is a term applied to asymptomatic CD patients with active SB lesions. Active SB lesions may be present even during asymptomatic clinical remission or when the patient has low levels of inflammatory markers. In 2015, Click et al. [13] linked elevated C-reactive protein (CRP) levels to ŌĆ£Silent CDŌĆØ in asymptomatic CD patients. They evaluated 351 asymptomatic CD patients with a 2-year observation period by classifying them into an elevated CRP group and a normal CRP group. CRP elevation was significantly associated with an increased risk of hospitalization (adjusted hazard ratio, 2.12; 95% CI, 1.13-3.98) in multivariate survival analysis. The same group also demonstrated by using the L├®mann Index that elevated CRP is independently associated with 7-fold greater worsening of the disease trajectory (OR, 6.93; 95% CI, 2.44-19.67) compared with a stable disease trajectory [14,15]. In my opinion, however, asymptomatic ŌĆ£Silent CDŌĆØ with CRP elevation is not actually ŌĆ£Silent CDŌĆØ because the increase in CRP, which is commonly measured in daily clinical practice, alerts the physician (especially IBD specialists) to the presence of an active lesion. We should be aware of ŌĆ£Real Silent CDŌĆØ in which CRP levels are not elevated. Approximately 50% of patients with normal CRP levels have an active lesion (as assessed by endoscopy) and 30% of patients are hospitalized for intestinal resection [13].
Korean investigators reported that half of the disease location sites in CD patients with normal CRP levels were in the ileum [16]. All operations related to ileocolonic or colonic lesions could be predicted by physicians whereas only 75% of the operations related to ileal lesions could be predicted. These authors concluded that CRP is less useful as a disease activity marker in patients with ileal CD than in those with ileocolonic or colonic CD. A Spanish group studied fecal calprotectin (FCP) levels in CD patients who had undergone ileocolonic resection [17]. In that study, the group with a Rutgeerts score of i2 had a median FCP level of 166.5 (interquartile range [IQR], 64.8-316.3) and a median CRP level of 0.45 (IQR, 0.11-0.62), and the group with an i3 score had a median FCP of 98.5 (IQR, 63-625) and a median CRP of 0.1 (IQR, 0.05-0.73).
Thus, CD patients with active SB lesions can exhibit ŌĆ£Real Silent CDŌĆØ coupled with a normal CRP or FCP range [18]. For this reason, I emphasize the importance of assessing SB lesions in patients with CD using imaging modalities such as endoscopy, magnetic resonance enterography (MRE), or ultrasound. The International Organization for the Study of IBD (IOIBD) states that although CRP and FCP are useful adjunctive biomarkers, they should not be used as treatment targets because normalization of these biomarkers alone is not sufficient [19].
OBJECTIVE MONITORING OF SB LESIONS IN PATIENTS WITH CD
Continuous adjustment of treatment depending on the results of scheduled objective monitoring is the key concept of the ŌĆ£treat-to-targetŌĆØ strategy [8]. The IOIBD states that ŌĆ£Endoscopy remains the gold standard for assessing location, depth, and extent of inflammatory mucosal lesions in CD.ŌĆØ [19] When endoscopy cannot adequately evaluate inflammation, however, cross-sectional imaging is necessary. In other words, crosssectional imaging and evaluation of biomarkers such as CRP and FCP are useful follow-up monitoring methods. Measurement of CRP or FCP levels cannot indicate the deformity, localization, distribution, or disability of CD lesions, but can provide complementary information. The appropriate method should be used at the appropriate time by considering the strengths and limitations of each monitoring method.
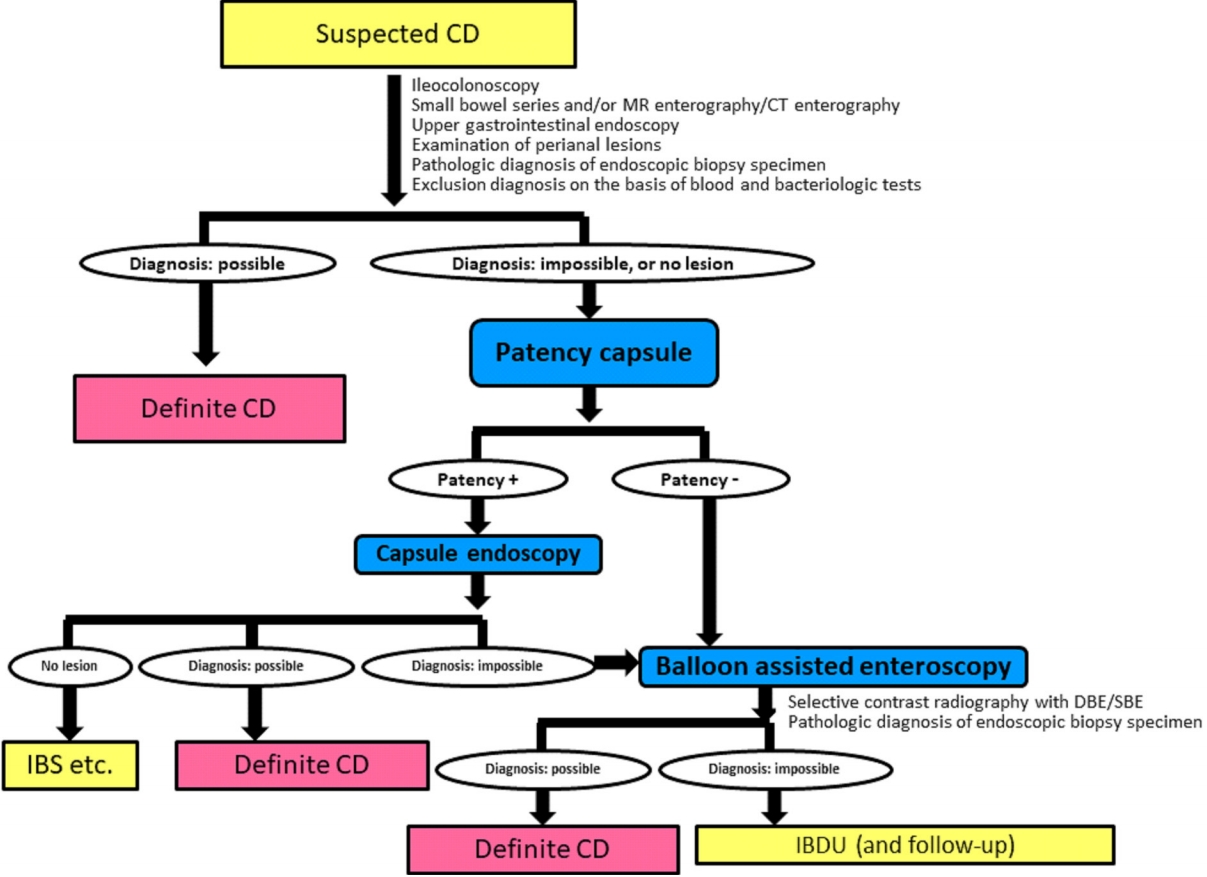
Monitoring CD by only conventional ileocolonoscopy is insufficient in cases of proximal ileum dominant or negative findings of conventional ileocolonoscopy at the initial diagnosis [20,21]. Fig. 1 shows the diagnostic strategy for achieving a definite diagnosis in difficult cases of patients with suspected CD using a patency capsule and subsequent capsule endoscopy (CE) or balloon-assisted enteroscopy (BAE) such as double balloon enteroscopy or single balloon enteroscopy [12]. This algorithm is applicable to patients with suspected CD. Ultrasound is a noninvasive monitoring modality for CD, but visualization of the proximal ileum is relatively difficult for technical reasons and the quality of visualization depends on the skill of the ultrasonographer [22,23]. MRE has several advantages and is globally recognized as a useful monitoring modality for the SB in patients with CD [24,25]. MRE is a noninvasive and radiation-free method for visualizing the layers of the intestinal wall and also permits visualization of extraintestinal findings in the abdomen. MRE, however, also has disadvantages. Gonz├Īlez-Su├Īrez et al. [26] reported that CE is superior to MRE for detecting lesions in all parts of the SB (jejunum, ileum, and terminal ileum). Further, MRE is less sensitive for detecting stenosis compared with BAE, especially for a thin stenosis without wall thickening, e.g., stricture formation as the result of mucosal healing after the administration of an anti-tumor necrosis factor (TNF)-╬▒ agent [27]. Cross-sectional imaging, such as ultrasound, computed tomography, enterography, or MRE, is superior to CE or BAE for assessing transmural inflammation. Transmural healing is a more ideal treatment goal beyond complete endoscopic mucosal healing in CD clinical practice. While complete endoscopic mucosal healing in the whole gastrointestinal tract is still the ideal goal, it is not easy to achieve in most CD patients, even in the era of biologics.
SB endoscopy is the most sensitive imaging modality for visualizing SB lesions in patients with CD [28]. Proactive management of CD patients was recently recognized as the optimal approach for avoiding disability and changing the natural progression of the disease compared with reactive management [29]. From this perspective, endoscopic monitoring is an ideal approach for proactively detecting changes in the disease progress within the subclinical phase. In 1990, Rutgeerts et al. [30] demonstrated that endoscopic recurrence develops prior to clinical recurrence in the neoterminal ileum after ileocecal resection. Endoscopic assessment and treating to target increase the likelihood of mucosal healing in patients with CD [31]. Of course, endoscopic examination of the SB has some limitations, such as potential capsule retention in CE, inability to achieve deep insertion in BAE due to severe adhesion or stenosis, and risk of perforation [9,32-35]. Appropriate use and secure confirmation of the functional patency of the intestinal tract using a patency capsule is essential to avoid capsule retention in CE [9,34]. In cases with stricture, ultrathin colonoscopy is sometimes useful for passing the stricture and observing the proximal lumen beyond the stricture [36]. Deep insertion should be cautiously performed in cases with higher active ileal lesions, especially those with longitudinal ulcers at the mesenteric site [9,32].
Some investigators or physicians mention invasiveness as a disadvantage of conventional ileocolonoscopy or BAE. While it is true that sedation is required for these endoscopic examinations, the balance between invasiveness and accuracy must be carefully considered. Inaccurate monitoring will provide insufficient information for decision-making in clinical practice. Each imaging modality and biomarker has its advantages and disadvantages. Objective monitoring procedures should be used appropriately on a case-by-case basis. Additionally, most patients will accept the risk of an invasive procedure if they are able to understand the value of the procedure for their clinical management [37]. Comparisons of the endoscopic picture between before and after treatment will help to demonstrate the efficacy of the treatment to the patient.
EFFICACY OF MEDICATION FOR SB LESIONS IN PATIENTS WITH CD
Is the efficacy of pharmacologic treatment for ileal lesions in patients with CD inferior to that for colonic lesions [38-40]? Reliable, precise, and objective procedures are needed to confirm the efficacy of each pharmacologic treatment for SB and colonic lesions. Further, for reliable translation from basic research, the mode of action for each drug must be carefully considered [41].
Most previous studies analyzed the data of the lesion location according to the Montreal classification [42,43]. Classification of the location, however, requires precise monitoring. More precise monitoring will likely result in an increase in the prevalence of SB lesion in patients with CD [44-47]. Therefore, I propose that clinical management and investigation depend on the dominancy of the location of CD lesions in the gastrointestinal tract. Recently, Dulai et al. [48] suggested a new classification for CD as either ileum dominant (isolated ileal and ileocolonic) or isolated colonic disease. However, I would like to advance the concept of a novel classification that depends only on location dominancy, as follows: jejunal dominant (rare); proximal ileum dominant; terminal ileum dominant; expanded SB dominant, in which lesions are distributed in more than 2 sections in the SB; colon dominant; and expanded SB-colon dominant (Table 1). The precision of imaging modalities is rapidly improving. Therefore, proactive clinical management should be performed. My proposed classification according to the dominance of the location of CD lesions capitalizes on the more detailed information provided by modern imaging modalities. In fact, my preliminary data revealed that 50% of lesions responsible for surgery were located in the small bowel (proximal to the terminal ileum) compared with 25% located in the ileocecal region, including the terminal ileum. Further studies are needed to confirm the utility of this novel classification.
ENDOSCOPIC BALLOON DILATATION AND SURVEILLANCE FOR SB LESIONS IN PATIENTS WITH CD
BAE has some advantages for the treatment of SB strictures in clinical practice. Endoscopic balloon dilatation (EBD) is widely performed to avoid surgery in daily clinical practice. Strictures in the proximal ileum or jejunum can usually be dilated only by BAE. Hirai et al. [49] investigated the efficacy and safety of EBD for SB strictures by BAE in a prospective multicenter study of patients with CD. Approximately 70% of the participants demonstrated short-term improvement in their symptoms and a larger dilatation diameter of the balloon was associated with the success of the procedure.
The short-term success of EBD depends on the patient selection with inclusion and exclusion criteria [9]. A long stricture ( Ōēź 5 cm), the presence of a fistula around the stricture, a severe angulated stricture, and a severe active lesion at the stricture site are contraindications for the procedure. Erosion at the stricture is not usually a contraindication, but the acceptable level of an active ulcer is controversial, as a shallow ulcer might not rule out dilation. Endoscopists should pay special attention to the presence of fissuring ulcers around the stricture site just before EBD by X-ray monitoring using a contrast agent. Fissuring ulcers are at very high-risk for perforation by EBD. The inclusion criteria for EBD are also controversial. EBD is indicated for CD patients with obstructive symptoms or a dilated intestine at the oral side of a stricture. CD patients with SB strictures without dilation at the oral side and no obstructive symptoms may undergo EBD at the discretion of the physician. In my clinical practice, strictures that cannot be passed through with an endoscope, even though without dilation at the oral side and without obstructive symptoms, are usually dilated to avoid the development of more severe strictures. Finally, multiple ileal strictures are often observed, and the number of strictures should be considered in the decision to perform EBD. To avoid surgery, all SB strictures should be dilated, but successful dilation of all SB strictures requires a highly skilled endoscopist due to the likelihood of severe adhesions.
The long-term efficacy of EBD is equally important for the patientŌĆÖs prognosis. Hirai et al. [50] previously demonstrated a cumulative surgery-free rate of 79% at 2 years and 73% at 3 years after the initial EBD. The cumulative redilation-free rate after initial EBD was 64% at 2 years and 47% at 3 years. The success of endoscopic dilation for all SB strictures and control of inflammation by medical treatment are key factors for avoiding hospitalization and surgery in the long-term. Ultimately, a treatto-target strategy with continuous precise objective monitoring and subsequent adjustment of the treatment content according to the results of the monitoring is important to avoid disabling states such as stricture formation [14]. In contrast, after stricture formation, BAE or surgery should be selected on a case-by-case basis because multiple factors, including the clinical characteristics, clinical treatment history, imaging findings of the stricture, and skills of the endoscopist, must be considered in the decision-making process [51].
CD-related SB cancer has a relatively low incidence in East Asia compared with Western countries [52]. BAE can be used to obtain biopsy tissue for surveillance. The endoscopic features of SB cancer are not yet well established because poorly differentiated adenocarcinoma or mucinous carcinoma is often observed in CD patients with CD-related SB cancer. The endoscopic findings of these cancers may differ from those of well-differentiated adenocarcinoma, similar to what is observed in colonic lesions in patients with ulcerative colitis [53]. SB strictures that are intractable to EBD are a risk factor and biopsy tissue should be obtained for surveillance [54].
CONCLUSIONS
Continuous and scheduled precise objective monitoring and adjustment of treatments are key factors in the treat-to-target strategy. Even if the short-term outcome is not significantly different from that of a non-treat-to-target group, the long-term outcome by the treat-to-target strategy should improve compared with the non-treat-to-target strategy [55]. For example, an adequate serum concentration of anti-TNF-╬▒ agent is variable depending on the situation: for remission induction, remission maintenance, or disease activity [56]. An optimal treatment strategy for SB lesions in patients with CD must be developed on the basis of reliable data obtained by precise and objective monitoring. Clinical management should be based on the dominant location of the intestinal lesions.