INTRODUCTION
The treatment of inflammatory bowel disease (IBD), including both ulcerative colitis (UC) and CrohnŌĆÖs disease (CD), is focused on clinical, endoscopic, and/or histological healing; and the importance of disease-related disability and quality of life is often underestimated [1]. Disability, as defined by the World Health Organization, includes impairments, limitations, and restrictions to perform/participate in an activity or involvement in life situations [2]. The concept of disability in IBD remained subjective until the development of IBD-specific disability indices in the last decade. The IBD disability index, a comprehensive 28-item validated questionnaire, remains the most commonly used index to assess disability in patients with IBD [3]. However, its complexity limits its use in routine clinical practice. To overcome this limitation, IBD-disk, a self-administered tool evaluating different dimensions of patient-reported outcome measures of quality of life was developed [4]. The IBD-disk has been recently validated in a large European IBD cohort [5].
The patient acceptability, understanding, and response to self-administered tools like IBD-disk are influenced by the local socio-cultural sensitivities and practices [6]. The universal application of IBD-disk therefore cannot be advocated until it is analyzed in different populations. We aimed to evaluate the real-life performance of the IBD-disk in assessing the IBD-related disability by correlating it with IBD daily life burden and the disease activity.
METHODS
1. Study Population
This is a cross-sectional study of patients with IBD (both UC and CD) who attended the outpatient clinic at Dayanand Medical College and Hospital Ludhiana, India between June 2021 and December 2021. Consecutive adult ( Ōēź 18 years) patients with an established diagnosis of IBD (based on European CrohnŌĆÖs and Colitis Organisation and the European Society of Gastrointestinal and Abdominal Radiology guidelines) [7] were asked to complete the standardized IBD-disk questionnaire. Patient demographics (age and sex) and disease characteristics (disease duration, classification, and activity) were recorded simultaneously. Non-consenting patients or patients who were unable to comprehend the IBD-disk questionnaire were excluded. The study was approved by the Institutional Ethics Committee (IEC No. DMCH/R&D/2020/23). All the authors had access to the study data.
2. IBD-Disk Tool
The IBD-disk includes 10 components (joint pain, abdominal pain, body image, education and work, emotions, energy, interpersonal interactions, regulation of defecation, sexual function, and sleep) (Supplementary Fig. 1). Each component is scored from 0 to 10 using a visual analogue scale (0, no disability; 10, maximal disability). The IBD-disk total score was calculated as the sum of the 10 individual component subscores (minimum score 0 and maximum score 100) [4,8,9]. An additional visual analogue scale was added to assess the IBD daily life burden (0 perfect and 10 worst, > 5 indicated high burden).
3. Assessment of Disease Activity
Patients with both UC and CD were classified according to the Montreal classification [10]. Disease activity was assessed using partial Mayo Clinic score (PMS) in patients with UC and Harvey Bradshaw Index (HBI) in patients with CD. Active UC was defined as PMS > 1 while active CD was defined as HBI Ōēź 5 [11-13].
4. Statistical Analysis
The quantitative data were expressed as mean ┬▒ standard deviation and the qualitative data as frequency. The associations between IBD-disk total score and patient and disease characteristics were evaluated using the MannŌĆÉWhitney test. A probability value of < 0.05 was considered statistically significant. SpearmanŌĆÖs correlation coefficient (Žü) was applied to assess the correlation between IBD-disk total score, IBD-disk subscores, IBD daily life burden, and disease activity. The values of Žü between 0.1-0.39, 0.40-0.69, 0.70-0.89, and Ōēź 0.90 were interpreted as weak, moderate, strong, and very strong correlations, respectively [14]. The internal consistency (or homogeneity) of the IBD-disk was assessed using CronbachŌĆÖs coefficient (╬▒). CronbachŌĆÖs ╬▒ > 0.7 and CronbachŌĆÖs corrected item correlation > 0.4 were considered significant. The area under the receiver operating characteristic (AUROC) curve was calculated to determine the accuracy of the IBD-disk total score to detect a high IBD daily life burden. All the statistical calculations were done using the SPSS version 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
During the study period, a total of 613 patients were asked to complete the IBD-disk questionnaire. After exclusion of the patients with incomplete questionnaires, 546 patients (84.9%; mean age, 40.33 ┬▒ 13.74 years, 282 males [51.6%]) were enrolled and analyzed. The majority of the patients (n = 464, 84.98%) had UC. Out of the 546 patients, 311 patients (56.95%) had the active disease (291 UC and 20 CD), while the remaining 235 patients (173 UC and 62 CD) were in remission. The baseline characteristics of the study population are summarized in Table 1.
1. Correlation between IBD-Disk and IBD Daily Life Burden
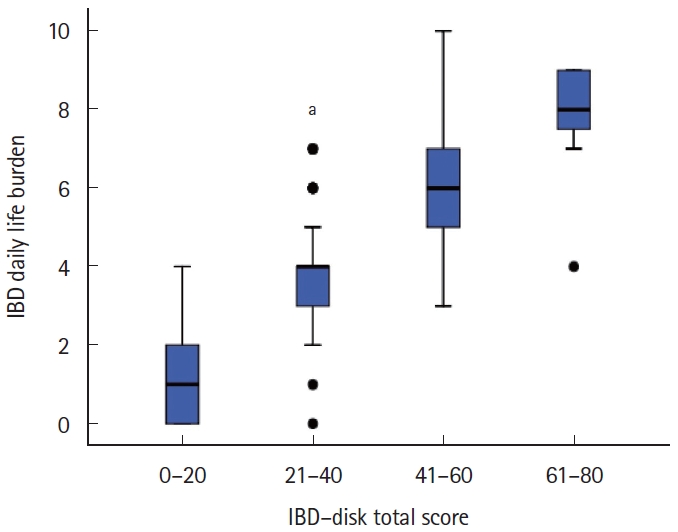
The mean IBD-disk total score of the enrolled patients was 18.39 ┬▒ 15.23. The mean IBD-disk subscores ranged between 0.07 (sexual functions) and 4.40 (energy). Forty-four patients (8.05%; 38 UC and 6 CD) had high IBD daily life burden. The mean IBD daily life burden score was 2.45 ┬▒ 2.02.
There was a strong correlation between the IBD-disk total score and the IBD daily life burden (Žü = 0.94, P< 0.001). The box plot of the distribution of the IBD daily life burden and the IBD-disk total score is depicted in Fig. 1.
On analyzing the subscores of the IBD-disk, 3 components (emotions, energy, and education and work) had a strong correlation, 6 components (abdominal pain, joint pain, body image, sleep, interpersonal interactions, and regulating defecation) had a moderate correlation while sexual functions had a weak correlation with the IBD daily life burden score. The correlations between IBD-disk subscores and IBD daily life burden in patients with UC and CD are summarized in Table 2. The correlations between IBD daily life burden, and abdominal pain, and emotions were significantly higher in females with IBD. On subgroup analysis, the IBD daily life burden in UC correlated significantly with abdominal pain, emotions and education and work in females. In patients with CD, however, no sex-based differences were observed in correlations of IBD-disk subscores and IBD daily life burden (Supplementary Table. 1).
2. Homogeneity of IBD-Disk
CronbachŌĆÖs ╬▒ calculated for the IBD-disk total score was 0.82. To test the contribution and consistency of the IBD-disk, one-at-a-time deletion of different items was done. The CronbachŌĆÖs ╬▒ (if item deleted) varied between 0.78 and 0.83 for all the 10 individual components of the IBD-disk. The corrected item-total correlations were > 0.4 for all the subscores except joint pain and sexual functions (Table 3). CronbachŌĆÖs ╬▒ was positive for each pair of IBD-disk components except (sexual function+sleep) and (sexual function+abdominal pain). The highest correlations were seen for (energy+emotions) and (emotions+body image) (Fig. 2).
3. Correlation between IBD-Disk and Disease Activity
The IBD-disk total score correlated moderately with PMS (Žü = 0.50) and weakly with HBI (Žü = 0.34). The IBD daily life burden score had a moderate correlation with both PMS (Žü= 0.48) and HBI (Žü= 0.41). Amongst the IBD-disk subscores, regulating defecation had the maximum correlation with both PMS and HBI (Supplementary Table. 2). Patients with active disease had higher mean values for the IBD-disk total score, IBD-disk subscores, and the IBD daily life burden as compared to patients who were in remission (Fig. 3).
The correlations of IBD-disk total score and subscores with IBD daily life burden were compared for patients with active disease and disease in remission. The IBD-disk total score correlated more strongly with IBD daily life burden in patients with UC in remission than patients with active UC, the difference being significant (0.95 vs. 0.91, P= 0.01 for UC and 0.93 vs. 0.92, P= 0.40 for CD). Except for energy in patients with UC and education and work for patients with CD, there was no effect of disease activity on the correlations of IBD-disk subscores with IBD daily life burden (Table 4).
4. Association between Disease Characteristics and Disability Assessed Using IBD-Disk and IBD Daily Life Burden
The IBD-disk or IBD daily life burden scores were not influenced by the type of IBD (UC or CD). The IBD-disk total score, IBD-disk subscores (except sexual function) and IBD daily life burden were higher in females (Table 5, Supplementary Table. 3).
A significant association of IBD-disk total score and IBD daily life burden was also observed with PMS in patients with UC and with HBI in patients with CD (Table 5). For both UC and CD, the mean IBD-disk scores increased with increasing disease activity (patients with mild disease activity had higher IBD-disk scores than patients in remission, but lower scores as compared to patients with moderate and severe disease). The trend was statistically significant (Table 5, Supplementary Table. 4).
There was no effect of age on the IBD-disk total score and IBD daily life burden. However, the mean IBD disk subscores of joint pains and sleep increased with increasing age. On subgroup analysis, younger adults (age < 40 years) with UC had higher mean scores for the body image subscore, as compared to older adults ( > 40 years) and elderly ( > 60 years). In contrast, older adults and elderly with CD had higher mean scores for joint pains (Supplementary Table. 5).
5. Diagnostic Accuracy of IBD-Disk
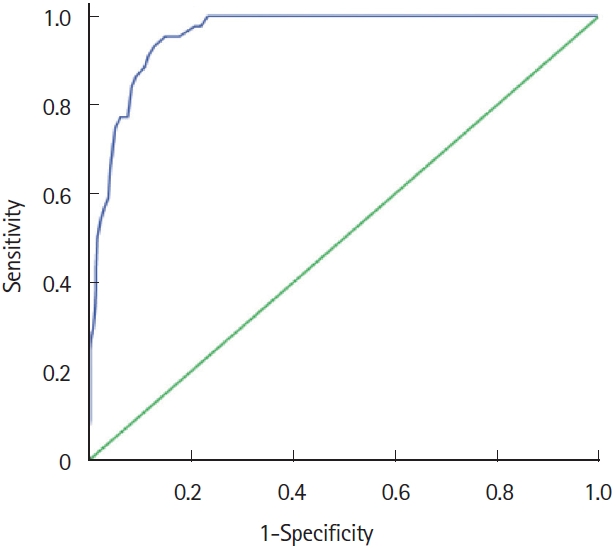
The diagnostic accuracy of the IBD-disk total score in predicting a high IBD daily-life burden ( > 5) was evaluated by calculating the AUROC, which was 0.96 (95% confidence interval, 0.94-0.98; P< 0.001) (Fig. 4). The threshold value for the IBD-disk total score to detect high IBD daily life burden was derived from coordinates of the receiver operating characteristic curve using the Youden Index. The IBD-disk total score > 30 predicted a high IBD daily life burden with a sensitivity of 95% and specificity of 85%.
DISCUSSION
For IBDs, patient-reported outcome measures evaluating both the disease activity as well as disability (and/or quality of life) are important to improve the long-term outcome and add value to the holistic IBD care. IBD disability index and IBD-disk are the 2 disability indices that have been validated in the European cohorts [3-5,15]. However, to ensure that the data captured by disability indices reflects the true picture, it is important that the survey tool is adapted to the respective populations. An ideal tool would perform uniformly across culturally diverse populations (cross-cultural equivalence) [16]. In the present study, we evaluated the real-world performance of IBD-disk to predict high IBD daily life burden in a large cohort of north Indian patients.
The mean IBD-disk total score was 18.39 ┬▒ 15.23 (range, 0-76). The IBD-disk total scores in the current study were lower than those reported in the west [5,8,9]. This could be attributed to either a differential perception of well-being or a true lower disability in the enrolled patients. The mean sexual function subscore was the lowest which is inconsistent with the impaired sexual function reported in IBD patients [17,18]. In the current study, only 4 participants (0.73%) reported a sexual function subscore of Ōēź 5 on the IBD-disk. Low sexual function scores could indicate hesitation on the part of patients in the current cohort to report their intimate experiences. Another IBD-disk component that scored low was the body image. There is evidence to suggest that body image dissatisfaction can negatively impact patients and is associated with poorer quality of life [19]. However, patients in the current study did not report any significant alteration in the perceived body image. In observant societies like India, therefore, the inclusion of sexual function and body image in the IBD-disk is expected to result in lower total and hence lower cutoff scores of the IBD-disk in predicting a high disability burden. This was observed in the current study where IBD-disk total score > 30 predicted high IBD daily life burden as compared to the threshold values of Ōēź 40, as described previously [8].
The IBD-disk total score correlated very strongly with IBD daily life burden (Žü= 0.94). There were no significant differences in the IBD-disk total score and IBD-disk subscores in patients with UC and CD, indicating a similar level of disability in both the types of IBD, consistent with the findings of the VALIDate study [5]. With a CronbachŌĆÖs ╬▒ of 0.82, the IBD-disk displayed good internal consistency to assess the disease-related disability.
The IBD-disk total score had a significant association with the female sex. Similar findings were also observed in the VALIDate study [5]. Higher disability scores in females are consistent with gender differences in the perception of psychosocial domains of disability. Depression, fatigue, and a lower quality of life have been reported more frequently in females [20,21]. The higher prevalence of extra-intestinal manifestations (such as arthralgia, arthritis, and osteopenia) in females and a social bias against females in conservative societies also contributes to higher disease-related disability in females.
Higher IBD-disk total scores were observed in patients with higher disease activity scores. Interestingly, the age, disease duration, extent, location, and behavior did not affect the disability scores. A total of 25 (16 UC and 9 CD) patients had IBD-disk total score > 30 despite the disease being in clinical remission. These observations suggest that nearly 1 in 7 patients with UC and one in 2 patients with CD have high disability despite the disease being in remission. The IBD-disk subscores that scored high in such patients were emotions, energy and sleep. The IBD-disk thus facilitates assessment of the ŌĆ£non-gastrointestinalŌĆØ disability experienced by such patients. Filling up the IBD-disk questionnaire by the patient at each visit to the healthcare facility, before seeing the treating physician, will allow a meaningful discussion between the two, focussing on the specific disability-related issues.
Although our study is limited by being a single-center study, the large sample size, with the disease spectrum mimicking the epidemiological characteristics of the local IBD population, is expected to reflect the actual burden of the disease. A greater number of patients in the current study had UC, as compared to the previous IBD-disk validation studies, where CD patients dominated the inclusion cohorts. Also, a majority of the patients enrolled in the current study had mild-moderate disease activity. This is also reflected in relatively infrequent use of biologics in the included cohort. The performance of IBD disk in patients with severe disease activity, hence, needs to be assessed in future studies, as disease activity is an important modifier of the disease-related disability. The IBD-disk tool was administered in the English language. Misinterpretation in patients not well versed or fluent in English cannot be ruled out, however, the proportion of such patients is expected to be very small. Translation and validation in regional languages are nevertheless required. As repeated assessments of the IBD-disk were not performed in the current study, the test-retest reliability could not be evaluated. This has, however, been reported earlier [22]. The long-term variability in IBD-disk scores also cannot be commented upon. The comparison of the IBD-disk with other disability indices such as IBD disability index was not done. Instead, IBD daily life burden was calculated using a unidimensional visual analogue scale. Similar approaches have been employed for other chronic diseases, and therefore the applicability of visual analogue scale in estimating the IBD daily life burden can be relied upon. The lack of endoscopic disease severity and inflammatory biomarkers such as fecal calprotectin or C-reactive protein did not allow objective assessment of the disease activity.
In conclusion, the IBD-disk is a consistent and accurate tool to determine IBD-related disability. It parallels the disease activity in patients with both UC and CD and is not affected by other disease characteristics, demonstrating the ubiquity of the tool, although gender specificity needs to be accounted for. The response to the IBD-disk is influenced by social and cultural beliefs. A universal cutoff of the IBD-disk cannot be recommended and population-specific thresholds thus need to be determined. Longitudinal studies with a more objective assessment of the disease activity and determinants of IBD-related disability are needed to evaluate the dynamicity of the IBD-disk in response to therapy.