INTRODUCTION
Inflammatory bowel disease (IBD) is a chronic non-specific intestinal disease mainly including CD and UC. The chronic, protracted course of IBD severely affects the patient's quality of life. The treatment of IBD has gone through 3 phases. Glucocorticoids were introduced in the 1950s, immunosuppressive agents began to be used in the 1960s, and therapeutics is now in the era of biological agents. With the progression and continuous standardization of its treatment, treatment efficacy for IBD has made great progress, resulted in significantly decreased complications and mortality in the patients. However, monotherapy or combination therapy with these drugs will change patient's immune status, which may bring corresponding issues, particularly an increased risk of opportunistic infection.1
Opportunistic infection refers to micro-organisms that have limited or no pathogenic capacity in healthy human bodies but cause diseases or induce infections when the immune system is compromised by other diseases (such as acquired immunodeficiency syndrome) or drug medications (such as immunosuppressive agents). IBD patients are high-risk populations for opportunistic infections. First, the disease itself can cause a reduced nutritional status in IBD patients. Second, the application of glucocorticoids, immunosuppressive agents, and biological agents can severely inhibit patient's immunity. Therefore, patients with IBD are susceptible to opportunistic infections, which requires much attention in clinical setting.2,3 The prevalence of various infectious diseases are relatively higher in China compared with those in the Western countries. Positive prevention, early diagnosis and timely control of opportunistic infections are the premise for improving the prognosis of IBD patients in China.4 This consensus referenced the results of clinical researches from both China and abroad, in combination with the characteristics of Chinese IBD patients, to provide guidance for clinical practices.
The IBD group of the Chinese Society of Gastroenterology, Chinese Medical Association organized the experts from the aspects of IBD, infection, clinical epidemiology and evidence-based medicine to establish this consensus using the Delphi method. Our IBD experts were divided into 7 research groups to perform literature retrieval, screening and assessments to confirm the patients-intervention-comparison-outcome issues that needed to be solved in the consensus. Three rounds of voting (with a total of 58 experts participating in it) were conducted through electronic mails, and the ballots were counted by a third party. Subsequently, in-person voting using a voting machine was conducted with a total of 24 experts. After 2 expert seminars, the draft was discussed, amended, and passed in the plenary meeting of the IBD group in China. After being reviewed and finalized by experts in the infection and clinical epidemiology, this consensus was finally established.
The 3 recommendation levels of this consensus are as follows: level A, where the rating standard a was passed by 3 out of 4 or higher voting; level B, where the rating standard a+b was passed by 3 out of 4 or higher voting; and level C, where the above-mentioned indicators were not reached and were deleted. The rating standards were: (1) total approval (indispensable, minimal requirement); (2) partial approval and recommendation (should be done, but did not reach the essential level); (3) depended on the conditions; and (4) disapproval (deleted, unreasonable, unnecessary, incompatible with national conditions, inoperatable, not assessable, and no need to include this item in the consensus).
Eight major topics, including cytomegalovirus (CMV) infection, Epstein-Barr virus (EBV) infection, viral hepatitis, bacterial infection, Mycobacterium tuberculosis infection, fungal infection, parasitic infection, and vaccines were discussed in this consensus (a total of 33 indicators) (Table 1).
IBD COMBINED WITH CMV INFECTION
1. The positive rate of serum anti-CMV IgG in IBD patients is higher than that in healthy controls
The epidemiology of CMV infection is associated with socioeconomy.5 Positive rate of serum CMV IgG in IBD patients has been reported to be high. For example, Yi et al.6 reported that serum CMV IgG positive rate was 73.54% in UC and 89.19% in CD patients in Wuhan (Hubei Province, China), while that in the healthy population was only 50.69%. However, CD patients are rarely infected with CMV, comprising of <5% of the reported cases.7
2. Screening for CMV infection is recommended for acute severe UC patients with glucocorticoid resistance
Many studies have noted that the rate of active CMV infection has been increasing in patients with severe UC and/or glucocorticoid resistance. According to the reports abroad, the percentages of CMV colitis in severe UC patients with glucocorticoid resistance ranged 20% to 40%,8 whereas that in UC patients who received emergency colectomy was 27%.9 Data from China showed that active CMV infection affected 46.2% of the severe UC patients receiving surgery10 and 36.7% of the refractory UC patients.11
3. Positive anti-CMV IgM and/or CMV pp65 antigenemia (âĽ1 CMV-positive cells out of every 150,000 white blood cells) and/or positive plasma CMV DNA in real-time quantitative PCR (qPCR) suggests active CMV infection
Several detection techniques are available for active CMV infections, each of them has its advantages and disadvantages. A combination application of various methods can increase the detection rate. (1) CMV-specific serum antibodies: including IgM and IgG. Serum IgM is mainly present after infected for 2 to 4 weeks; therefore, its early diagnostic value is limited.12,13 (2) CMV pp65 antigenemia assay: its sensitivity and specificity are 60% to 100% and 83% to 100%, respectively.14 The disadvantage of the assay is that it cannot distinguish latent infection from active infection, and the result is affected by the reduced peripheral neutrophil count. (3) Culture of viruses: the specificity of the culture is high (89%-100%), but with a relatively low sensitivity (45%-78%),13 and it is not widely applied in clinical setting. (4) qPCR detection of plasma and fecal CMV DNA: the sensitivity and specificity of the test to diagnose active infection using qPCR for plasma CMV DNA range 65% to 100% and 40% to 92%, respectively.14,15 The sensitivity of CMV DNA in stool samples using qPCR is high.16
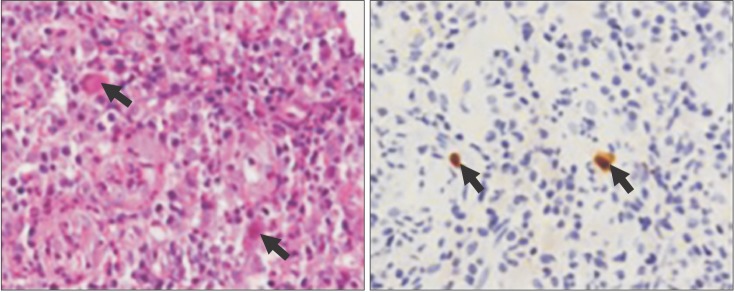
4. Gold standard for diagnosing CMV colitis is positive histopathology by H&E stain combined with positive immunohistochemistry (IHC) and/or positive qPCR for CMV DNA in colonic mucosal tissues
(1) The sensitivity of HE stain is low (range, 10%-87%); therefore, the early diagnostic value of the test is limited. However, its specificity reaches 92% to 100%.17,18,19 When giant cells, intranuclear inclusion bodies, perinuclear halo, and owl's eye-like changes are observed (Fig. 1), CMV colitis can be diagnosed.20,21 (2) IHC stain of colonic mucosal tissues has a high sensitivity (78%-93%)22 and is the gold standard for the diagnosis of CMV colitis. (3) Detection of CMV DNA in colonic mucosal tissues using qPCR has a sensitivity of 92.0% to 96.7% and a specificity of 93.0% to 98.7%.
5. Antiviral therapies should be considered in cases with peripheral CMV DNA >1,200 copies/mL by qPCR
Yang et al.23 applied the receiver operating characteristic (ROC) curve analysis to determine the threshold value of 1,150 copies/mL to detect CMV DNA using qPCR and showed that the sensitivity and specificity for the diagnosis of CMV colitis were 44.4% and 78.9%, respectively.
6. Typical colonoscopic features including mucosal defect, punched-out ulcer, longitudinal ulcer, cobblestone-like changes and irregular ulcer suggest CMV Colitis, routine biopsy and differential diagnosis should be performed
Wide mucosal defect, punched-out ulcer, longitudinal ulcer, cobblestone-like changes and irregular ulcer might be characteristic endoscopic features of CMV colitis. Suzuki et al.24 showed that the sensitivity and specificity of longitudinal ulcer in the prediction of CMV colitis reached 100% and 95%, respectively. Yang et al.23 reported that UC patients with CMV colitis can present with punched-out ulcer, irregular ulcer and cobblestone-like changes.
7. Antiviral therapy should be initiated in time in severe steroid-resistant colitis patients with CMV colitis. Discontinuation and dose reduction of immunosuppressive agents should be considered based on the evaluation of pros and cons
There is evidence indicating that CMV, as a hidden factor, can aggravate the disease in patients with refractory UC.12,25,26 After antiviral therapy, the clinical remission rate reaches 67% to 100%, and the mortality rate is reduced from 71% to 14.5%-17.6%.8,27
The consensus of the European Crohn and Colitis Organization (ECCO) recommends that when severe UC patients with glucocorticoid resistance have combined CMV colitis, antiviral therapy should be administered; the cessation of immunosuppressive agents is also recommended.28 However, one study suggested that when glucocorticoids or immunosuppressive agents are discontinued, the severity of UC was aggravated.29 Therefore, individualized assessment should be performed on the basis of patient's condition.
8. A 3- to 6-week course of antiviral therapy for patients with IBD combined with CMV colitis is recommended
The major drugs for treating IBD combined with CMV colitis are ganciclovir and foscarnet sodium.30 Ganciclovir is given at a dose of 5 mg/kg twice daily via intravenous infusion, and the treatment course is usually no less than 3 weeks. Valganciclovir is the prodrug of ganciclovir. Its bioavailability is good by oral administration. After absorption, it is phosphorylated to form ganciclovir triphosphate, which has an efficacy equivalent to that of ganciclovir. The routine dose of the drug is 900 mg twice daily, and it can be administered orally as maintenance therapy. The efficacy of foscarnet sodium is equivalent to that of ganciclovir, and is intravenously administrated at 180 mg/kg/day. The drug administration is divided into 2 to 3 doses, and the treatment course is usually no less than 3 weeks.
IBD COMBINED WITH EBV INFECTION
9. IBD patients who present active EBV infection during the administration of immunosuppressive agents are recommended to weigh the pros and cons for discontinuing immunosuppressive agents
Several studies have indicated that IBD patients are at a risk of developing lymphoma, especially those who receive mercaptopurine treatment, some might be associated with EBV infection.31,32,33 When IBD patients treated with immunosuppressive agents are suspected to have EBV infection, blood routine examination, peripheral blood smear, liver function test and serological indicator for EBV should be closely monitored. For patients with previously negative EBV serology, the presence of elevated EBV DNA titers might indicate the risk of developing lymphoproliferative diseases.34 The primary treatment is to reduce the dose of or discontinue immunosuppressive agents. After immunosuppressive agents are discontinued, EBV-related lymphoproliferative diseases can usually be spontaneously relieved.35
10. Hematologists should be consulted for the diagnosis and treatment of EBV-related lymphoproliferative diseases
IBD patients who have active EBV infection poorly responded to antiviral therapy (acyclovir and ganciclovir), while antiviral therapy is ineffective when EBV-related lymphoproliferative diseases are present.34 Discontinuation of immunosuppressive agents might lead to a spontaneous regression of EBV-related lymphoproliferative diseases.35,36 In the absence of spontaneous regression or progression after the withdrawal of immunosuppressive agents, rituximab monoclonal antibody can be considered for CD20-positive B cell lymphoma. In addition, patients with EBV infection should be highly alerted to the development of macrophage activation syndrome (MAS) and hemophagocytic lymphohistiocytosis (HLH). Once EBV infection combined with MAS/HLH or EBV-related lymphoproliferative diseases occurs, close collaboration and correspondence with hematologists are recommended to establish reasonable diagnostic and therapeutic strategies.
IBD COMBINED WITH VIRAL HEPATITIS
11. All IBD patients should be tested for HBsAg, anti-HBs and anti-HBc. Those with positive HBsAg and anti-HBc should be further tested for HBeAg, anti-HBe and HBV DNA
Foreign studies have reported 6 cases of IBD patients exhibiting HBV reactivation during the administration of glucocorticoids and/or thiopurines, 5 of whom developed liver failure.37,38,39 HBV reactivation in IBD patients caused by infliximab (IFX) has also been reported.40 A clinical survey of IFX application in China showed that 3 out of 4 HBsAg-positive patients presented elevated ALT while using IFX.41 Therefore, HBV screening is recommended to be performed when IBD is initially diagnosed rather than after immunosuppressive agent therapy is initiated.42,43,44,45 Since occult infection carries a risk of HBV reactivation, further HBV DNA screening has been recommended for patients with negative HBsAg and positive anti-HBc.38
12. Prophylactic antiviral therapy with nucleos(t)ide analogues is recommended prior to the use of immunomodulators in HBsAg-positive IBD patients regardless of HBV DNA levels. Antiviral therapy should be started 1-2 weeks before the treatment with glucocorticoids and immunosuppressive agents and should last for at least 12 months after the cessation of immunosuppressive agents
HBV reactivation rate has been reported to be 16% to 36% in HBsAg-positive IBD patients. The reactivation risk is associated with long-term (>3 months) combined (âĽ2) application of immunosuppressive agents without receiving prophylactic antiviral therapy.45 Lamivudine is the most commonly used prophylactic antiviral drug for IBD; however, its 1-year and 5-year drug resistance rates are up to 30% and 70%, respectively.46 Long-term anti-tumor necrosis factor (anti-TNF) therapy can further increase the drug resistance rate.47,48 Therefore, lamivudine is currently recommended for short-term treatment only. For IBD patients, the influence of antiviral therapy on the immunosuppressive treatment should be avoided as much as possible. Therefore, tenofovir and entecavir, which have low drug resistance rates and strong antiviral effects, are recommended.28,49,50 The risk of developing liver cirrhosis and hepatocellular carcinoma (HCC) in chronic hepatitis B with HBV DNA >2,000 IU/mL is significantly increased; therefore, patients with HBV DNA >2,000 IU/mL should continue antiviral therapy. The endpoint of treatment is the same as that of the general hepatitis B population.28,51,52
13. HCV is not an absolute contraindication to immunosuppressive therapy but should be closely monitored due to a high risk of HCV reactivation
In 2014, Huang et al.53 reported that HCV infection rate in IBD patients was not statistically different from that in the general population. Among 714 IBD patients, the HCV infection rate was 0.42%, while that in the non-IBD patients was 0.36% (P =0.80). This result was consistent with another Italian study.54
The use of glucocorticoids and immunosuppressive agents in IBD patients may affect the disease course of hepatitis C. Loras et al.38 reavealed that the use of glucocorticoids might result in massive replication of HCV and liver damage. Brunasso et al.55 analyzed 37 relevant studies in 153 HCV-infected patients who received IFX for rheumatoid arthritis and showed that only one exhibited definite hepatic aggravation. Current data has shown the acceptable safety of anti-TNF therapy in HCV-infected IBD patients.45,55
14. Whether interferon (IFN), the commonly used anti-HCV medication, will aggravate IBD remains unclear. The risk of IBD aggravation by anti-HCV therapy and the interaction among drugs should be fully considered. Direct-acting antiviral agents (DAAs) for anti-HCV therapy are recommended
Currently, the major anti-HCV regimen in China is the PR regimen, consisting of pegylated interferon Îą (PEG IFN-Îą) combined with ribavirin.56 This regimen is applicable to all HCV genotypes when there are no contraindications. A newly developed mediation, anti-HCV DAAs, is already on the Western markets, but this type of drugs is still under clinical trial in China. Before they receive antiviral therapy for HCV infection, the risk of IBD aggravation by antiviral therapy and the possible interactions among drugs should be fully considered.45
IBD COMBINED WITH BACTERIAL INFECTION
15. When IBD patients have combined active bacterial infections, immunosuppressive agents should be reduced or even discontinued based on patient conditions, and sensitive antibiotics should be chosen
Both immunosuppressive and biological agents can cause immune decline, when IBD patients have combined active bacterial infections, immunosuppressive agents should be temporarily suspended, and sensitive antibiotics should be applied.28
16. IBD is an independent risk factor of Clostridium difficile infection
C. difficile is a type of Gram-positive, spore-forming, anaerobic bacillus that is a common opportunistic pathogen of nosocomial infections. C. difficile can induce diarrhea, pseudomembranous colitis and severe sepsis. The risk factors of C. difficile infection include antibiotic exposure, low immunity, long-term hospitalization and advanced age.57,58 Studies from the Western world have shown that IBD, especially UC, is an independent risk factor of C. difficile infection.28 A single-center, retrospective study suggested that C. difficile infection rate is significantly increased in IBD patients; in particular, those with active disease and colonic involvement are prone to be infected with C. difficile.59
17. Hand hygiene is important for preventing nosocomial infection of C. difficile
There are many transmission vectors of C. difficile , among which transmission by hand is an important route.60 Protection through the use of gloves or hand hygiene is important for preventing nosocomial infection. Prevention with drugs is currently not recommended for C. difficile infection. Guo et al.61 compared the effects of 5 different hand hygiene methods for removing C. difficile on hands, showing that general liquid soap had the best effect on C. difficile , followed by antibacterial liquid soap, quaternary ammonium salt disinfecting wipes, running water, and the 6-step hand-hygiene technique using an alcohol-based rapid hand-disinfection solution. Isolation of the patient is recommended to prevent the transmission of infection within the hospital if C. difficile infection is confirmed or suspected.62
18. In IBD patients receiving glucocorticoids or immunosuppressive agents exhibit disease recurrence or unsatisfactory treatment response, screening for C. difficile is recommended
IBD patients with long-term use of glucocorticoids or immunosuppressive agents are at a significantly increased risk of C. difficile infection that may aggravate the severity of the disease. A large-scale study based on the general population showed that, regardless of doses and treatment courses, the risk of C. difficile infection in IBD patients treated with glucocorticoids was increased by 3.4-fold compared with those receiving immunosuppressive and biological agents.63 Long-term use of immunosuppressive agents also increases the risk of C. difficile infection in IBD patients,64 while long-term application of biological agents does not.63
19. Tests for C. difficile detection include the detection of dehydrogenase antigen, toxins A/B by ELISA, bacterial culture, cytotoxicity assay and nucleic acid amplification technology (NAT)
The detection of C. difficile detection includes the following 3 methods: (1) detection of toxins A/B of C. difficile in stool samples or via the cytotoxicity neutralization assay (CCNA); (2) detection of the bacterium, such as the detection or culture of glutamate dehydrogenase (GDH); (3) detection of toxin genes using NAT.65 Xu et al.66 compared the 3 detection methods (C. difficile stool culture, nucleic acid PCR, and detection of toxin A/B using ELISA) and demonstrated that the sensitivity of nucleic acid PCR and ELISA toxin detection was not significantly different from that of anaerobic culture.
There are many methods for the diagnosis of C. difficile infection, among which detecting toxin B of the bacterium using CCNA is the gold standard. Combination use of NAT and ELISA for combined detection is generally recommended. Endoscopic examination is generally not used as an essential detection method for C. difficile infection.
20. The treatment for IBD patients combined with C. difficile infection may refer to that in non-IBD patients; metronidazole or oral vancomycin is recommended. For patients with severe C. difficile infection, vancomycin has a better efficacy than metronidazole and is recommended as the preferred choice
Metronidazole is the preferred choice of treatment for C. difficile infection, including recurrent infections.67 Metronidazole is generally given orally at a dose of 200 to 250 mg 4 times/day or 400 to 500 mg thrice daily fora total treatment course of 10-14 days. Vancomycin can be used for treating recurrent or metronidazole-ineffective C. difficile infection.68 A meta-analysis has shown that the efficacy of treating mild-to-moderate C. difficile using vancomycin or metronidazole was not significantly different from that of using other antibiotics (such as rifaximin).69,70,71 However, for patients with severe C. difficile infection or have aggravated symptoms after treated with metronidazole, vancomycin is recommended to be given as soon as possible.72 For acute C. difficile infection, oral administration of vancomycin at the dose of 125 mg every 6 hours is recommended.72 To prevent the recurrence of C. difficile infection, gradually reducing the dose of vancomycin or using intermittent medication is recommended. The specific usage is the oral administration of 125 to 500 mg every 3 days for 2 to 3 weeks.68 Other antibiotics such as nitazoxanide and rifaximin are mainly used for recurrent C. difficile infection.73 Intravenous administration of tigecycline is effective for severe, complicated, and recurrent C. difficile infection.74
21. For IBD patients combined with C. difficile infection, the pros and cons should be considered for the use of immunosuppressive agents
The application of thiopurines in IBD patients can increase the risk of C. difficile infection.75 If antibiotics only are used and without the administration of immunosuppressive agents, the above-mentioned risk is not increased. If immunosuppressive agents are used in combination, such risk might be further increased.76 Therefore, whether IBD patients combined with C. difficile infection should continue using immunosuppressive agents or not would be considered based on the evaluation of the pros and cons of treatment efficacy and the adverse consequences caused by C. difficile infection.
IBD AND M. tuberculosis INFECTION
22. TNF-Îą antagonists can cause reactivation of latent tuberculosis infection (LTBI) or increase the risk of tuberculosis infection;77 therefore, screening for tuberculosis should be routinely performed prior to the initiation of TNF-Îą antagonists
Recent studies have shown that some IBD patients (1.65%) still develop tuberculosis even after LTBI screening before the use of TNF-Îą antagonists;78 these patients are prone to develop extra-pulmonary tuberculosis that presents as fever, elevated CRP and low positive rate of pathogen detection.79 IBD patients with LTBI should be given anti-tuberculosis therapy for at least 3 weeks before the administration of TNF-Îą antagonists. And patients should avoid biological agent treatment within 3 months after receiving M. tuberculosis vaccination.28,80,81 During the TNF-Îą antagonist therapy, tuberculosis infection should be monitored by evaluating patient's clinical presentations and chest X-ray examination every 8 to 16 weeks.82,83
23. Screening of tuberculosis is recommended prior to the use of glucocorticoids, purines or methotrexate
It has been shown that the application of glucocorticoid equivalent to prednisone âĽ15 mg/day for more than one month can increase the risk of LTBI.84,85,86 Using purines alone can also increase the risk of LTBI reactivation.87,88 The combination of purines with glucocorticoids and/or TNF-Îą antagonists is more likely to cause LTBI reactivation than purines monotherapy.
24. Recommendation for screening active tuberculosis or LTBI: past history of tuberculosis infection or contact, chest X-ray examination, pure protein derivative (PPD) test and/or interferon-Îł release assays (IGRAs) should be performed. The efficacy of IGRAs in the diagnosis of LTBI is better than the PPD test; therefore, IGRAs should be the first diagnostic modality of choice under certain circumstances
Patients' past history of tuberculosis infection or contact, the presence of tuberculosis poisoning symptoms and chest X-ray results should all be considered in screening active tuberculosis infection.28,89,90 Current screening methods for LTBI include the tuberculin skin test (TST) and IGRAs (quantiFERON-TB Gold and T-SPOT.TB). Neither TST nor IGRAs can distinguish between LTBI and active tuberculosis. Many studies have shown that IGRAs are better than TST in cases received BCG inoculation, those with a contact history of active tuberculosis, high-risk medical workers and children infected with tuberculosis.91,92,93,94,95,96,97 Considering China as a country with heavy tuberculosis burden, the Chinese Society for Tuberculosis, Chinese Medical Association recommends both PPD and IGRAs to be adopted for screening LTBI in China. Patients with a positive PPD test can be further evaluated by IGRAs for further confirmation. Patients with autoimmune diseases or organ transplantation should receive IGRAs alone or in combination with PPD tests for screening LTBI before receiving glucocorticoids or TNF-Îą antagonists.98
25. Before LTBI patients receive TNF-Îą antagonists or glucocorticoids (equivalent to prednisone âĽ15 mg/day), the treatment with 1 to 2 anti-tuberculosis drugs for 3 weeks is recommended. This antituberculosis regimen should continue for 6 months during the TNF-Îą antagonists or glucocorticoid therapy
For IBD patients having LTBI who are being treated with TNF-Îą antagonists or glucocorticoids, the following prophylactic anti-tuberculosis strategies are recommended: isoniazid 0.3 g/day and rifampin 0.45 g/day for 6 months, or isoniazid 0.9 g/week and rifapentine 0.9 g/week for 3 to 6 months. Whether prophylactic anti-tuberculosis treatment is required for IBD patients with previous tuberculosis should be individualized based on patients' past treatments and discussions with specialists.99
26. When active tuberculosis is diagnosed, the standardized anti-tuberculosis therapy should be started immediately, and TNF-Îą antagonists and immunosuppressive agents (such as purines and methotrexate) should be discontinued. The pros and cons of continuous use of glucocorticoids in this situation should be weighed or decided after discussion with specialists
Currently, there has been no recommendation for a standard regimen and treatment course of anti-tuberculosis therapy targeting immunosuppressed hosts. Patients are recommended to be transferred or referred to tuberculosisspecific hospitals or to receive medications under the guidance of tuberculosis specialists. Patients with treatmentnaive tuberculosis can be given the 2HRZE/4HR regimen (H, isoniazid; R, rifampicin; Z, pyrazinamide; E, ethambutol) for 6 months according to the recommendations of the World Health Organization (WHO) and the Chinese guidelines for the prevention and treatment of pulmonary tuberculosis. Patients with recurrent pulmonary tuberculosis are provided with the 3HRZES/6HRE regimen (S, streptomycin) for 9 months. Patients with tuberculous pleuritis are given the 2HRZE/10HRE regimen for 12 months. Because IBD patients infected with active tuberculosis are mainly exhibiting opportunistic infection in an immunosuppressive host, the 2HRZE/10HRE anti-tuberculosis regimen for 12 months is recommended.
27. Biological agents can be restored after 2-3 months of standard anti-tuberculosis therapy and tuberculosis-related indicators are improved when required when active TB is diagnosed
According to the London consensus of the World Congress of Gastroenterology on biological therapy for IBD80 and the ECCO consensus on IBD opportunistic infection,28 the restoration of TNF-Îą antagonists is recommended to be considered after 2 to 3 months of standard anti-tuberculosis therapy and when the patient's tuberculosis-related indicators are improved. Currently, there is no evidence showing the appropriate timing to restore immunosuppressive agents in IBD patients who are infected with tuberculosis; the patient's overall condition should be considered, and the consensus on biological agents may be used as a reference.
IBD COMBINED WITH FUNGAL INFECTION
28. Fungi are resident flora in the human gastrointestinal tract that play important roles in intestinal homeostasis. Their functions in the development of IBD are still not clear; they might be able to become opportunistic pathogens in IBD patients
When human immunity decreases (e.g., after treated with immunosuppressive agents and glucocorticoids and in the presence of gene mutations in effector molecules including Dectin-1 and CARD9) and/or the fungal load increases (such as with the use of large amounts of antibiotics that causes intestinal flora disturbance, thus resulted in excessive fungal growth), normal fungal flora in the intestine and other locations may turn into pathogens, inducing fungal infectious diseases and even lethal invasive fungal infection.100,101,102,103,104
29. Once IBD patients have a combined invasive fungal infection, drugs that suppress human immunity should be stopped in principle, and anti-fungal treatment should be started in a timely manner
Based on the different locations of infections and disease severity, treatment strategies for fungal infection also differ. Focal superficial fungal infections usually require local application of anti-fungal drugs, whereas disseminated fungal infections usually require the intravenous administration of anti-fungal drugs. Based on such situations, surgical debridement and immunotherapy may also be required.105,106
Once invasive fungal infection is confirmed, drugs that suppress human immune functions should be stopped in principle, including glucocorticoids, immunosuppressive and biological agents. If fungal infection is only superficial (such as local skin infection), local anti-fungal drugs can effectively control the disease; whether immunosuppressive agents should be stopped remains controversial and requires a careful assessment of IBD severity and the pros and cons of continuous therapy. However, the risk of continuous application of anti-TNF preparations is high.
IBD COMBINED WITH PARASITIC INFECTION
30. Specific screening for parasitic infections before the application of immunosuppressive agents is not considered necessary unless the patients are long-time residents of or have travelled to epidemic areas
There are relatively fewer studies on IBD combined with parasitic infection. Currently, there is no clear evidence supporting routine screening for parasites. If patients are long-time residents of or have travelled to an epidemic area, screening can be considered conditionally. If patients are suspected to have a combined parasitic infection, immunosuppressive agents can be reduced accordingly. After the infection is controlled and IBD needs to be treated using immunosuppressive agents in a patient, secondary prevention can be performed based on the opinions of infectious disease specialists.
VACCINATION IN IBD PATIENTS
31. Live attenuated vaccines are contraindications to those patients with IBD under the use of immunosuppressants
IBD patients exhibit dysregulated immune responses after treatment with immunosuppressants. Vaccines for preventing against pathogens of opportunistic infection can be considered.107,108 If the inoculation of live attenuated vaccines is required during the immunosuppressive agent treatment, glucocorticoids are recommended to be discontinued for 1 month and immunosuppressive agents for more than 3 months. If the inoculation of live attenuated vaccines is required before using immunosuppressive agents, the drugs should be postponed for at least 3 weeks.
32. If IBD patients have a negative HBV serology (both anti-HBs and anti-HBc are negative), medical therapy can be started, and inoculation of HBV vaccine is recommended
For IBD patients with negative HBV serology (both anti-HBs and anti-HBc are negative), inoculation of HBV vaccine (recombinant [yeast] hepatitis B vaccine) is recommended to be given at the time of IBD diagnosis.51,109
The HBV vaccine inoculation procedure involves several steps. A double-dose inoculation and/or re-inoculation procedure may be preferential, that is, 3 doses of 40 Âľg recombinant hepatitis B vaccine are inoculated at 0, 1 and 2 months at the first vaccination, and anti-HBs needs to be re-examined within 1 to 3 months after the last shot. Patients with anti-HBs <100 IU/L must receive the second round of vaccination. The total response rate after 2 inoculations is 57% to 79%.110,111 Moreover, other guidelines also recommend receiving another 3 doses if the first inoculation fails.112,113
Screening anti-HBs levels every 6 to 12 months has been recommended to determine the immunosuppressive status, and those with anti-HBs <10 IU/L should receive one booster shot. However, there is no relevant recommendation for IBD patients.112,114
Regarding the inoculation time, the short course (0, 1 and 2 months) allows immunosuppressive patients to obtain immune protection as soon as possible, whereas the long course (0, 1 and 6 months) yields higher antibody titers but increases the risk of HBV infection in patients with delayed immune responses.112 In addition, a four-shot inoculation (0, 1, 2 and 6 months) may increase the immune response,112 although this strategy requires further studies in IBD patients.
Regarding antibody titers for IBD patients, anti-HBs level >10 IU/L is considered to confer effective immune protection.111 However, for high-risk populations, such as patients with immunosuppressive status and chronic diseases (including IBD), anti-HBs >100 IU/L is considered to confer effective serological protection.115,116
33. IBD patients can be inoculated with the pneumococcus vaccine
PPV23 is a 23-valent polysaccharide vaccine targeting Streptococcus pneumonia that contains up to 98% of S. pneumoniae serotypes that cause pneumonia. PPV23 stimulates excellent immune functions in clinical trials in IBD patients.117 ECCO consensus recommends inoculating the PPV23 pneumococcus vaccine 2 weeks before the initiation of treatment in IBD patients to prevent infection with S. pneumonia.28