.
. .
.INTRODUCTION
Ulcerative colitis (UC) is a chronic inflammatory disease of the colon characterized by alternating periods of relapse and remission.1 Although the incidence and prevalence rates of IBD in the Asia-Pacific region are low compared with those in the Western Hemisphere,2 epidemiological studies have shown that the incidence and prevalence rates of UC are increasing in East Asia.2,3,4,5,6,7
Additional challenges for the effective management of UC in East Asia include delay in diagnosis and access to appropriate and affordable treatment, as well as the high prevalence of infectious diseases (e.g., hepatitis B and tuberculosis) in some Asian countries.8 Furthermore, there are limited studies evaluating population-specific issues of UC in East Asia, and patients and physicians require greater access to relevant information about available treatments and knowledge of the disease. Consequently, additional treatment options are needed for UC in East Asia, along with studies assessing their efficacy and safety in this patient population.7
Tofacitinib is an oral, small-molecule Janus kinase inhibitor that is being investigated for UC. The efficacy and safety of tofacitinib for UC have been reported in a global phase 2 dose-finding study,9 2 identical global phase 3 induction studies (OCTAVE Induction 1 and 2), and 1 global phase 3 maintenance study (OCTAVE Sustain).10
In the 8-week tofacitinib induction trials OCTAVE Induction 1 and 2,10 significantly higher proportions of patients treated with tofacitinib 10 mg twice daily (BID) achieved remission at week 8 (placebo-adjusted rate of remission across OCTAVE Induction 1 and 2, 11.6%) and mucosal healing at week 8 (placebo-adjusted rate, 16.3%) compared with placebo-treated patients. In the 52-week maintenance trial OCTAVE Sustain,10 significantly higher proportions of patients who received tofacitinib 5 mg BID and tofacitinib 10 mg BID achieved remission at week 52 (placebo-adjusted rates, 23.2%-29.5%), mucosal healing at week 52 (placebo-adjusted rates, 24.2%-32.6%), and sustained corticosteroid-free remission among patients in remission at the study baseline (placebo-adjusted rates, 30.3%-42.2%), compared with patients who received placebo. The long-term safety of tofacitinib 5 mg BID and 10 mg BID is being evaluated in an ongoing open-label extension study (OCTAVE Open, NCT01470612).
We evaluated the efficacy and safety of tofacitinib in the subpopulation of patients from East Asia enrolled in the OCTAVE Induction and OCTAVE Sustain randomized controlled trials.
METHODS
1. Patients
Efficacy and safety data from East Asian patients (patients from study centers in Japan, Korea, and Taiwan) who participated in 2 phase 3 induction studies of tofacitinib for UC (OCTAVE Induction 1 [NCT01465763] and OCTAVE Induction 2 [NCT01458951]) and 1 phase 3 maintenance study (OCTAVE Sustain [NCT01458574]) are presented. The inclusion and exclusion criteria in these studies have been reported previously for the global population.10 Briefly, patients in OCTAVE Induction 1 and 2 had moderately to severely active UC, and must have failed or been intolerant to therapy with at least 1 of the following: corticosteroids, azathioprine, 6-mercaptopurine, or anti-tumor necrosis factor (anti-TNF) therapies (infliximab or adalimumab).
Patients who completed OCTAVE Induction 1 and 2 with clinical response (Ōēź3 points and Ōēź30% decrease from baseline in Mayo score with accompanying decrease in rectal bleeding subscore of Ōēź1 point or absolute rectal bleeding subscore Ōēż1) were eligible to participate in the 52-week tofacitinib maintenance study, OCTAVE Sustain.
2. Study Design
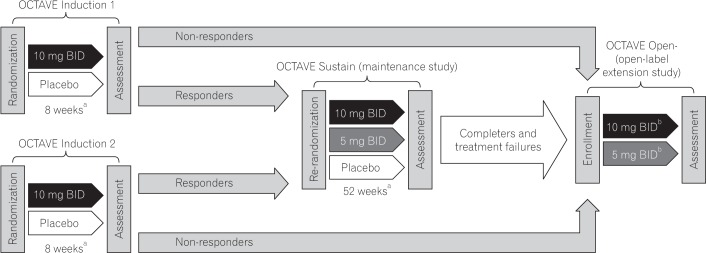
OCTAVE Induction 1 and 2 were identically designed, randomized, double-blind, placebo-controlled studies. Eligible patients were randomized (1:4) to treatment with placebo or tofacitinib 10 mg BID for 8 weeks (Fig. 1). OCTAVE Induction 1 and 2 initially included a tofacitinib 15 mg BID treatment arm that was removed after a protocol amendment. OCTAVE Sustain was a randomized, double-blind, placebo-controlled study in which eligible patients were re-randomized (1:1:1) to receive placebo, tofacitinib 5 mg BID, or tofacitinib 10 mg BID for 52 weeks.
3. Efficacy and Safety Evaluations
1) Efficacy
The full details of the efficacy evaluations performed in OCTAVE Induction 1, OCTAVE Induction 2, and OCTAVE Sustain have been reported previously.10 In OCTAVE Induction 1 and 2, the primary end point was remission (total Mayo score Ōēż2, with no individual subscore >1, and rectal bleeding subscore 0) at week 8, and mucosal healing (endoscopic subscore 0 or 1) at week 8 was the key secondary end point. In OCTAVE Sustain, remission at week 52 was the primary end point. The key secondary end points in OCTAVE Sustain were mucosal healing at week 52 and sustained (achieving remission at both weeks 24 and 52) corticosteroid-free (not requiring corticosteroids for Ōēź4 weeks before each visit) remission among patients in remission at baseline. The other efficacy end points assessed in OCTAVE Induction 1, OCTAVE Induction 2, and OCTAVE Sustain included the proportions of patients with clinical remission (total Mayo score Ōēż2, with no individual subscore >1), endoscopic remission (endoscopic subscore 0), and change from baseline in partial Mayo score (Mayo score excluding the endoscopic findings subscore).
Health-related quality of life was assessed using the patient-reported Inflammatory Bowel Disease Questionnaire (IBDQ).11 The change from baseline in total and individual domain scores was assessed along with IBDQ remission (defined as total IBDQ score Ōēź170) and IBDQ response (Ōēź16 points increase from the baseline IBDQ total score).
Efficacy data at week 8 of OCTAVE Induction 1 and 2 were used as baseline data in OCTAVE Sustain.
2) Safety
Adverse events (AEs) and clinical laboratory parameters were recorded throughout the studies. Follow-up was up to week 13 post-baseline of OCTAVE Induction 1 and 2 for patients who were not transferred into the maintenance study (OCTAVE Sustain) or the open-label extension study (OCTAVE Open), and week 57 post-baseline of OCTAVE Sustain for patients who were not transferred into OCTAVE Open.
4. Statistical Analysis
In these post-hoc analyses, data from patients enrolled at East Asian (Japan, Korea, and Taiwan) study centers are presented. For OCTAVE Induction 1 and 2, pooled data are presented. Efficacy data are presented for the full analysis set, which included all patients randomized to placebo, tofacitinib 5 mg BID (OCTAVE Sustain only), or tofacitinib 10 mg BID. For the binary efficacy end points, subjects with missing data were treated as non-responders (non-responder imputation). Safety data are presented for all randomized patients who received at least 1 dose of study drug.
Descriptive statistics are presented for patients receiving placebo, tofacitinib 5 mg BID (OCTAVE Sustain only), and tofacitinib 10 mg BID. Treatment differences and 95% CIs were calculated using the normal approximation for the difference in binomial proportions. Data from the 3 East Asian patients (all of whom were from Japan) randomized to tofacitinib 15 mg BID in OCTAVE Induction 1 and 2 were not included in the induction study efficacy and safety evaluation. The primary efficacy analyses in OCTAVE Sustain included patients who received tofacitinib 15 mg BID in the induction study. A sensitivity analysis was performed for analysis of binary clinical efficacy end points in OCTAVE Sustain, in which patients who received tofacitinib 15 mg BID in the induction study were excluded. These 3 patients were included in the OCTAVE Sustain safety evaluations.
5. Study Ethics and Patient Consent
These studies were conducted in compliance with the Declaration of Helsinki and the International Conference on Harmonization Good Clinical Practice Guidelines, and were approved by the institutional review boards and/or independent ethics committees at each of the investigational centers participating in the studies or a central institutional review board. All patients provided written informed consent.
RESULTS
1. Patients
Globally, 1,207 patients were randomized in OCTAVE Induction 1 and 2 (including patients randomized to tofacitinib 15 mg BID). This subpopulation analysis included 121 patients from East Asia who were randomized and treated in OCTAVE Induction 1 and 2 (62 patients from Japan, 57 from Korea, and 2 from Taiwan). Twenty-six patients received placebo and 95 received tofacitinib 10 mg BID. One patient (3.8%) receiving placebo and 6 patients (6.3%) receiving tofacitinib 10 mg BID dropped out of the study (Fig. 2A). Patient demographics and baseline disease characteristics are presented in Table 1. Approximately two-thirds (65.4%-66.3%) of patients had extensive disease or pancolitis. Among the East Asian subpopulation, 51.6% to 53.8% had prior anti-TNF failure and 28.4% to 34.6% were using oral corticosteroids at baseline.
A total of 593 patients were re-randomized globally in OCTAVE Sustain, of whom 63 were from East Asia (39 from Japan, 23 from Korea, and 1 from Taiwan). Twenty patients received placebo, 22 received tofacitinib 5 mg BID, and 21 received tofacitinib 10 mg BID. Eleven patients (55.0%) receiving placebo, 6 (27.3%) receiving tofacitinib 5 mg BID, and 7 (33.3%) receiving tofacitinib 10 mg BID discontinued (Fig. 2B). Insufficient clinical response (including discontinuation because of worsening UC, i.e., UC flare) was the most frequent reason for discontinuation in all treatment groups (placebo, n=10; tofacitinib 5 mg BID, n=6; tofacitinib 10 mg BID, n=6). The demographics and baseline disease characteristics of patients in OCTAVE Sustain were generally balanced across treatment groups (Table 1). The majority of patients (81.8%-90.5% across treatment groups) receiving tofacitinib 10 mg BID during OCTAVE Induction 1 and 2, and numerically fewer patients (15.0%) randomized to receive placebo in OCTAVE Sustain, were in remission at maintenance study baseline compared with patients randomized to tofacitinib 5 mg BID (40.9%) and tofacitinib 10 mg BID (38.1%).
2. Efficacy
1) Efficacy in OCTAVE Induction 1 and 2
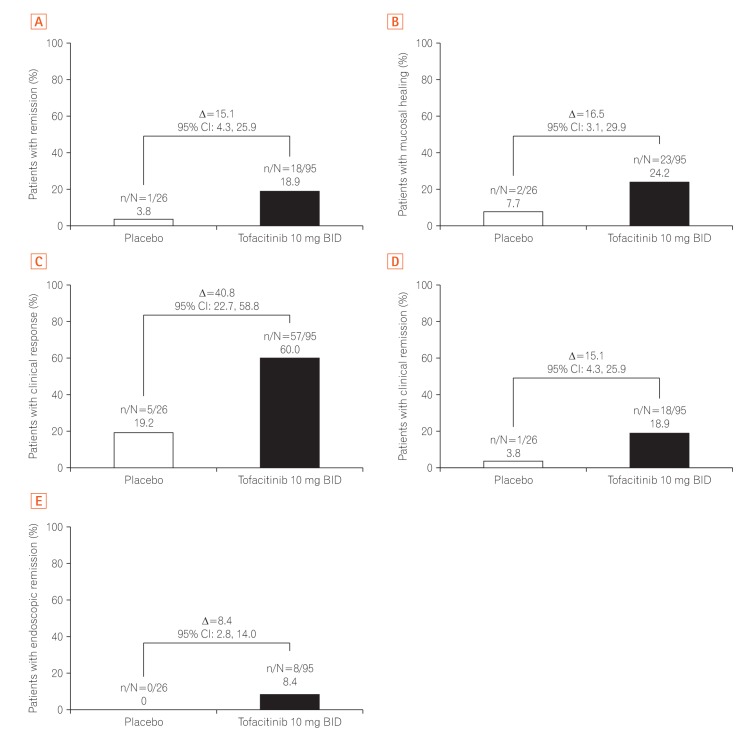
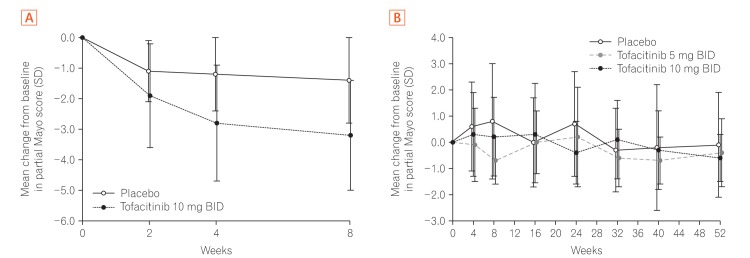
A numerically greater proportion of East Asian patients receiving tofacitinib 10 mg BID (18/95, 18.9%) achieved the primary end point of remission at week 8 versus placebo-treated patients (1/26, 3.8%; difference from placebo [95% CI]: 15.1% [4.3, 25.9]) (Fig. 3A). For the key secondary end point of mucosal healing at week 8, the response rate with tofacitinib 10 mg BID (23/95, 24.2%) was numerically greater than with placebo (2/26, 7.7%; difference from placebo [95% CI]: 16.5% [3.1, 29.9]) (Fig. 3B). The clinical response rate at week 8 was 60.0% (57/95) with tofacitinib 10 mg BID versus 19.2% (5/26) with placebo (difference from placebo [95% CI]: 40.8% [22.7, 58.8]) (Fig. 3C). Compared with placebo-treated patients, a numerically greater proportion of tofacitinib-treated patients achieved clinical remission (18/95 [18.9%] with tofacitinib vs. 1/26 [3.8%] with placebo; difference from placebo [95% CI]: 15.1% [4.3, 25.9]) (Fig. 3D) and endoscopic remission (8/95 [8.4%] with tofacitinib vs. 0/26 [0%] with placebo; difference from placebo [95% CI]: 8.4% [2.8, 14.0]) (Fig. 3E) at week 8. The mean change from baseline in partial Mayo score was greater for patients receiving tofacitinib 10 mg BID versus those receiving placebo at week 2 (first post-baseline assessment), week 4, and week 8 (Fig. 4).
2) Efficacy in OCTAVE Sustain
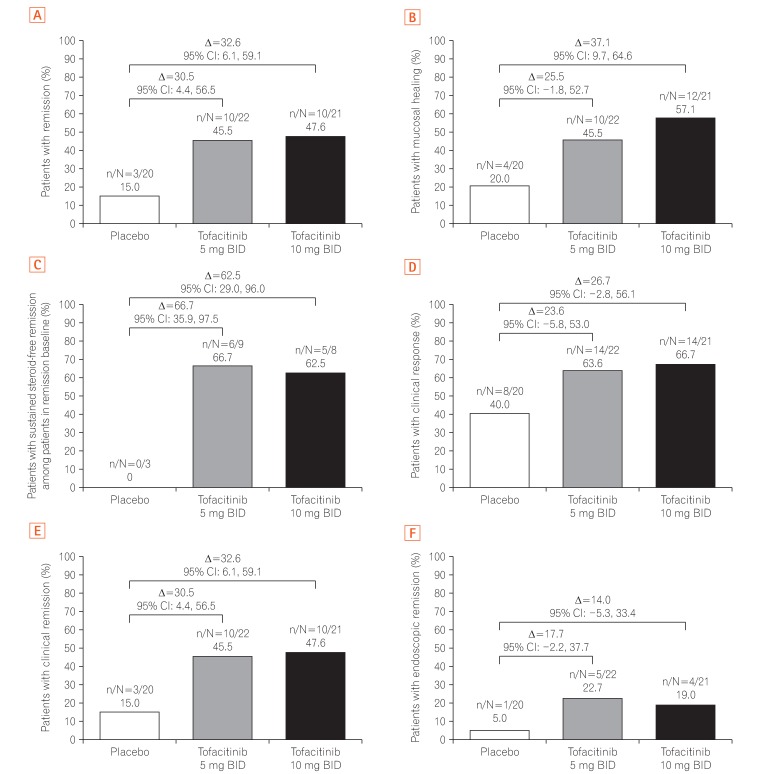
A numerically greater proportion of East Asian patients receiving tofacitinib 5 mg BID (10/22, 45.5%) and tofacitinib 10 mg BID (10/21, 47.6%) achieved the primary end point of remission at week 52 versus placebo-treated patients (3/20, 15.0%) (Fig. 5A). The difference from placebo (95% CI) was 30.5% (4.4, 56.5) with tofacitinib 5 mg BID and 32.6% (6.1, 59.1) with tofacitinib 10 mg BID. In the sensitivity analysis excluding patients who received tofacitinib 15 mg BID in the induction study, 9 of 21 (42.9%) patients in the tofacitinib 5 mg BID group and 9 of 20 (45.0%) patients in the tofacitinib 10 mg BID group achieved remission at week 52 versus 3 of 19 (15.8%) patients in the placebo group. The difference from placebo (95% CI) for the sensitivity analysis was 27.1% (0.3, 53.8) with tofacitinib 5 mg BID and 29.2% (1.9, 56.5) with tofacitinib 10 mg BID (Supplementary Fig. 1A). Mucosal healing at week 52 was achieved by numerically greater proportions of patients receiving tofacitinib 5 mg BID (10/22, 45.5%; difference from placebo [95% CI]: 25.5% [ŌłÆ1.8, 52.7]) and tofacitinib 10 mg BID (12/21, 57.1%; difference from placebo [95% CI]: 37.1% [9.7, 64.6]) versus those receiving placebo (4/20, 20.0%) (Fig. 5B). In the sensitivity analysis, mucosal healing at week 52 was achieved by 9 of 21 patients (42.9%) in the tofacitinib 5 mg BID group (difference from placebo [95% CI]: 21.8% [ŌłÆ6.2, 49.8]) and 11 of 20 (55.0%) patients in the tofacitinib 10 mg BID group (difference from placebo [95% CI]: 33.9% [5.5, 62.4]), compared with 4 of 19 (21.1%) patients with placebo (Supplementary Fig. 1B). Sustained steroid-free remission among patients in remission at baseline was achieved by numerically greater proportions of patients receiving tofacitinib 5 mg BID (6/9, 66.7%; difference from placebo [95% CI]: 66.7% [35.9, 97.5]) and tofacitinib 10 mg BID (5/8, 62.5%; difference from placebo [95% CI]: 62.5% [29.0, 96.0]) compared with placebo (0/3, 0%) (Fig. 5C). In the sensitivity analysis, sustained steroid-free remission among patients in remission at baseline was achieved by 5 of 8 (62.5%) patients receiving tofacitinib 5 mg BID (difference from placebo [95% CI]: 62.5% [29.0, 96.0]), 5 of 8 (62.5%) patients receiving tofacitinib 10 mg BID (difference from placebo [95% CI]: 62.5% [29.0, 96.0]), and none of 3 (0%) patients receiving placebo (Supplementary Fig. 1C).
In the primary analysis, the rates of clinical response (Fig. 5D), clinical remission (Fig. 5E), and endoscopic remission (Fig. 5F) at week 52 were numerically greater with both doses of tofacitinib versus placebo, with similar results obtained for the sensitivity analysis (Supplementary Fig. 1D-F).
Improvements in partial Mayo score gained during OCTAVE Induction 1 and 2 were maintained across all treatment groups in OCTAVE Sustain (Fig. 4B).
3. Patient-Reported Outcomes
1) Patient-Reported Outcomes in OCTAVE Induction 1 and 2
The baseline (SD) mean IBDQ total score was 129.0 (29.4) in the placebo group and 135.8 (28.9) in the tofacitinib 10 mg BID group. Treatment with tofacitinib 10 mg BID resulted in numerically greater improvements from baseline versus placebo in the IBDQ total score and in all IBDQ domain scores at weeks 4 and 8. The mean change from baseline in total IBDQ score with tofacitinib 10 mg BID was 22.5 at week 4 and 27.4 at week 8. The respective values with placebo were 11.5 and 14.9. For the Bowel Function Score, the week 8 mean change from baseline was 10.6 with tofacitinib 10 mg BID versus 6.6 with placebo (week 4: 8.5 vs. 4.7, respectively). For the Emotional Status Score, the mean changes from baseline were 7.5 versus 5.0 at week 8 and 6.6 versus 4.6 at week 4 for tofacitinib 10 mg BID and placebo, respectively. The respective changes from baseline in the Systemic Symptoms Score were 4.3 versus 2.1 at week 8 and 3.3 versus 0.9 at week 4. For the Social Function Score, the changes from baseline were 5.1 versus 1.2 at week 8 and 4.1 versus 1.3 at week 4 in the tofacitinib and placebo groups, respectively. IBDQ remission at week 8 was achieved by 56.8% of tofacitinib-treated patients versus 15.4% of patients with placebo (44.2% vs. 19.2% at week 4), and IBDQ response at week 8 was achieved by 62.1% of tofacitinib-treated patients versus 38.5% of those with placebo (55.8% vs. 34.6% at week 4).
2) Patient-Reported Outcomes in OCTAVE Sustain
The mean (SD) IBDQ score at baseline of OCTAVE Sustain was 164.0 (26.8) in the placebo group, 174.0 (10.9) in the tofacitinib 5 mg BID group, and 166.4 (18.8) in the tofacitinib 10 mg BID group. The mean changes from baseline in the total IBDQ score at week 52 of OCTAVE Sustain were 3.1 with tofacitinib 5 mg BID and 9.9 with tofacitinib 10 mg BID, compared with ŌłÆ1.0 with placebo. The mean changes from baseline in the Bowel Function Score at week 52 were ŌłÆ0.8 with tofacitinib 5 mg BID, 3.4 with tofacitinib 10 mg BID, and 0.8 with placebo. For the Emotional Status Score, the week 52 mean changes from baseline were 3.4 and 3.0 with tofacitinib 5 mg BID and 10 mg BID, respectively, versus ŌłÆ1.3 with placebo. For the Systemic Symptoms Score, the mean changes from baseline at week 52 were 0.3 with tofacitinib 5 mg BID, 1.5 with tofacitinib 10 mg BID, and ŌłÆ0.8 with placebo. For the Social Function Score, the week 52 changes from baseline were 0.1 and 2.1 with tofacitinib 5 mg BID and 10 mg BID, respectively, and 0.3 with placebo. At week 52 of OCTAVE Sustain, 50.0% of patients in the tofacitinib 5 mg BID group, 42.9% of patients in the tofacitinib 10 mg BID group, and 15.0% of patients in the placebo group achieved IBDQ remission. IBDQ response at week 52 was achieved by 40.9% and 52.4% of patients receiving tofacitinib 5 mg BID and tofacitinib 10 mg BID, respectively, versus 30.0% of patients receiving placebo.
4. Safety
The proportion of East Asian patients in OCTAVE Induction 1 and 2 who experienced AEs was similar for the group receiving tofacitinib 10 mg BID versus those receiving placebo (Table 2). Two patients experienced serious AEs (SAEs) with tofacitinib treatment during OCTAVE Induction 1 and 2: 1 patient experienced 1 SAE (Clostridium difficile infection) and 1 patient experienced 2 SAEs (UC and condition aggravation). There was 1 SAE (anal fistula) in the placebo group. One patient in the tofacitinib treatment group discontinued owing to an AE, versus none in the placebo group.
In OCTAVE Sustain, the proportion of patients who experienced AEs was numerically higher with both doses of tofacitinib versus placebo. There were 3 SAEs in OCTAVE Sustain: 2 with placebo (diverticulitis in 1 patient and venous embolism in 1 patient) and 1 with tofacitinib 5 mg BID (lumbar vertebral fracture). One patient in the placebo group discontinued because of an AE, and there were no discontinuations owing to AEs with tofacitinib 5 mg BID or tofacitinib 10 mg BID.
In OCTAVE Induction 1 and 2, infections occurred more frequently with tofacitinib treatment (22.1%) than with placebo (11.5%). One serious infection (Clostridium difficile) occurred in the tofacitinib treatment group versus none in the placebo group. In OCTAVE Sustain, infections were more frequent with tofacitinib 5 mg BID (59.1%) and tofacitinib 10 mg BID (47.6%) than with placebo (30.0%). There was 1 serious infection in the placebo group (diverticulitis) versus none with either dose of tofacitinib.
There was one adjudicated opportunistic infection in East Asian patients during OCTAVE Induction 1 and 2. The patient was receiving tofacitinib 10 mg BID and experienced an AE of herpes zoster (non-serious and moderate in severity) on day 22 of the study, which was adjudicated as an opportunistic infection based on multidermatomal involvement. The patient did not discontinue tofacitinib, and completed the study. There were no East Asian patients with opportunistic infections in OCTAVE Sustain, and none had herpes zoster AEs.
There were no intestinal perforation AEs, adjudicated cardiovascular events, adjudicated malignancy events, tuberculosis events, or deaths with tofacitinib treatment in the East Asian population of patients in OCTAVE Induction 1 and 2 and OCTAVE Sustain.
Changes from baseline in clinical laboratory parameters in the East Asian patient population during OCTAVE Induction 1 and 2 and OCTAVE Sustain are summarized in Table 3. Across all studies, there were increases from baseline in total cholesterol, LDL, HDL, and CK with tofacitinib treatment compared with placebo. Changes from baseline in triglycerides, the ratio of total cholesterol to HDL, and the ratio of LDL to HDL were generally similar between treatment groups, and there were no meaningful changes in other clinical laboratory parameters, including hemoglobin levels, absolute lymphocyte and neutrophil counts, and aminotransferase levels. No rhabdomyolysis, myopathy, or cases of drug-induced liver injury (potential Hy's law cases) were reported in tofacitinib-treated patients.
DISCUSSION
In these post-hoc analyses of East Asian patients enrolled in global phase 3 induction and maintenance studies of tofacitinib for moderately to severely active UC, oral tofacitinib 10 mg BID demonstrated numerically greater efficacy versus placebo in inducing remission, mucosal healing, clinical response, clinical remission, and endoscopic remission at week 8 in East Asian patients. Support for the early onset of treatment effect with tofacitinib 10 mg BID was demonstrated by numerically greater improvements from baseline of OCTAVE Induction 1 and 2 in partial Mayo score as early as week 2 (first post-baseline assessment), and at weeks 4 and 8. In OCTAVE Sustain, efficacy in remission, mucosal healing, sustained steroid-free remission among patients in remission at baseline, clinical response, clinical remission, and endoscopic remission end points was observed at week 52 with tofacitinib 5 mg BID and tofacitinib 10 mg BID, with numerically greater response rates with both doses of tofacitinib versus placebo. Tofacitinib also improved healthrelated quality of life versus placebo, as demonstrated by improvements in patient-reported end points derived from the IBDQ at weeks 4 and 8 in OCTAVE Induction 1 and 2, and at week 52 in OCTAVE Sustain. The efficacy of tofacitinib 5 mg BID and tofacitinib 10 mg BID in the East Asian population was generally consistent with that observed in the overall global OCTAVE Induction 1, OCTAVE Induction 2, and OCTAVE Sustain study populations.10
During the 8-week induction studies and 52-week maintenance study, the safety profile of tofacitinib 5 mg BID and tofacitinib 10 mg BID in East Asian patients was largely consistent with the results of the global analysis.10 There were no new or unexpected safety signals in the East Asian patient population, neither with respect to the global study population nor compared with tofacitinib treatment in other disease populations, including rheumatoid arthritis,12 psoriasis,13 and Crohn's disease.14 During OCTAVE Induction 1 and 2, the rates of AEs and SAEs were similar between the tofacitinib and placebo treatment groups; SAEs and discontinuations because of AEs were infrequent. In OCTAVE Sustain, the proportion of patients with AEs was numerically greater in the tofacitinib treatment groups than in the placebo group, and the SAE rates were similar across treatment groups. A numerically greater proportion of patients discontinued owing to insufficient clinical response in OCTAVE Sustain with placebo than with tofacitinib 5 mg BID and tofacitinib 10 mg BID. As in the global analyses, in East Asian patients, infections occurred more frequently in all studies with tofacitinib 5 mg BID and tofacitinib 10 mg BID than with placebo, and there were treatment-related increases in the levels of serum lipid parameters.
The treatment effect sizes observed with tofacitinib in the East Asian OCTAVE Induction 1 and 2 population for clinical remission, mucosal healing, and clinical response end points were broadly in line with the range reported for induction therapy in global studies of infliximab,15 adalimumab,16 and vedolizumab17 for the treatment of UC. Similarly, the treatment effect sizes with tofacitinib in East Asian patients at week 52 of OCTAVE Sustain were comparable to those reported in the maintenance phases of infliximab,15 adalimumab,16 and vedolizumab17 studies.
Importantly, the OCTAVE studies included a more stringent definition of remission, in which patients were required to have a rectal bleeding subscore of 0 in addition to the requirements for clinical remission (total Mayo score Ōēż2 and no individual subscore >1) in the studies of infliximab, adalimumab, and vedolizumab.15,16,17 The safety profile of tofacitinib in the East Asian population was similar to that observed in these global studies of anti-TNF therapies,15,16 in which similar rates of AEs and SAEs and higher rates of infections were observed with active treatment versus placebo. In the vedolizumab study,17 the rates of infections and serious infections were not different between treatment groups.
The efficacy of tofacitinib demonstrated in these analyses of East Asian patients is in contrast to that observed with adalimumab in a study of 273 Japanese patients with moderately to severely active UC.18 In this study of anti-TNF-naive patients refractory to corticosteroids and/or immunomodulators, the remission rates at week 8 with 2 dose regimens of adalimumab were not different from those with placebo. Furthermore, the magnitude of treatment effect observed in other end points in the adalimumab study was lower than that observed for the equivalent end points with tofacitinib.18 The safety profile of adalimumab observed in the Japanese study was broadly consistent with that observed with tofacitinib in these analyses, with similar rates of AEs and SAEs across treatment groups and a greater rate of infections with active treatment versus placebo.
A limitation of these analyses was that the East Asian patient population was relatively small, and the comparison of efficacy and safety between the treatment groups was based on descriptive statistics only. In addition to the relatively small sample size in these East Asian analyses, the 1:4 randomization ratio resulted in a small number of patients in the placebo groups of OCTAVE Induction 1 and 2. Thus, the ability to detect and compare AEs with low occurrence rates was limited. An ongoing open-label extension study (OCTAVE Open, NCT01470612) will allow further characterization of the long-term safety profile of tofacitinib.
In conclusion, in the East Asian population of patients in OCTAVE Induction 1 and 2, tofacitinib 10 mg BID was efficacious and well tolerated as an induction therapy for moderate to severe UC. In East Asian patients in OCTAVE Sustain, tofacitinib 5 mg and tofacitinib 10 mg BID demonstrated greater observed treatment effects versus placebo as maintenance therapy. No new safety signals were observed. The efficacy and safety of tofacitinib in East Asian patients were generally consistent with observations in the global study populations, and we detected no difference in the response of East Asian patients to tofacitinib therapy compared with the overall study populations.