INTRODUCTION
Ulcerative colitis (UC) is a chronic inflammatory condition of the colorectum that is characterized by relapsing and remitting cycles [1]. Medical treatment of UC is divided into induction and maintenance therapies. While the main target of induction therapy is achieving mucosal healing, the ultimate goal in patients with refractory UC is to avoid surgery. However, more than 20% of patients with UC are obliged to undergo total colectomy during their clinical course [2]. Despite the recent increase in treatment options for refractory UC, most of these medications cause immunosuppression, raising concerns about the increased risk of serious infections, especially in older patients. Thus, additional therapeutic options with a new mode of action and minimal safety concerns are warranted for better clinical outcomes in refractory UC.
Indigo naturalis (IN), also referred to as Qing-Dai, is extracted from the leaves and stems of plants, including Indigofera tinctoria and Strobilanthes cusia. Indigo and indirubin molecules, which are the main components of IN, were reported to be endogenous human aryl hydrocarbon receptor (AhR) ligands [3]. AhR signaling was reported to improve colitis in mice via interleukin-22 (IL-22) [4] by promoting mucosal healing [5]. IN also ameliorated murine DSS-induced colitis by upregulating IL-10 and IL-22 via AhR activation [6]. The regulation of host-microbiota communication was suggested to be a potential mechanism related to mucosal healing by AhR signaling [7,8].
Several studies have demonstrated the favorable efficacy of IN to induce remission in UC [9,10], and IN was suggested to be the choice of induction therapy for such patients. Conversely, IN is not generally considered an herbal medicine for longterm use. However, our previous retrospective study suggested the possible maintenance effect of IN in refractory UC [11]. Therefore, we conducted this prospective study with different participants to determine the clinical efficacy and safety of IN as maintenance therapy for patients with UC. In this study, we also assessed the influence of IN maintenance therapy on mucosal microbiota using mucosal biopsy samples, on the basis that induction therapy by IN might modify the fecal microbiota composition [10].
METHODS
1. Study Entry Criteria
This prospective uncontrolled open-label study was conducted at Kyushu University Hospital. We recruited subjects with UC who fulfilled both the inclusion and exclusion criteria, as described below. The diagnosis of UC was confirmed by the criteria established by the Japanese Ministry of Health, Labour, and Welfare [12]. The inclusion criteria were as follows: (1) patients aged Ōēź 16 years; (2) moderate to severe active UC (clinical activity index [CAI] Ōēź 8 and Mayo endoscopic subscore [MES] Ōēź 2); (3) left-sided or extensive UC; and (4) no history of IN treatment. The exclusion criteria were as follows: (1) pregnant or breastfeeding women; (2) patients with psychosomatic disorders, liver, or renal disease; and (3) patients with thrombocytopenia or taking antithrombotic therapy.
2. Study Protocol
Powdered IN was purchased from Seishin-shoyakudo (Tokyo, Japan). Each patient took 1 g of IN capsules twice a day (2 g/day orally). When adverse events (AEs) that were possibly related to IN occurred during the study period, the daily dose of IN was reduced as appropriate in the attending physiciansŌĆÖ discretion. No increase in the dosage of concurrent medications and no additional treatment for UC was allowed within 2 weeks before the study baseline. During the study period, concurrent medications could be reduced or stopped based in the attending physiciansŌĆÖ discretion. However, when the dosage of concurrent medications was increased or new medications were added, the patient was considered to have exacerbated UC.
The clinical disease activity was assessed by trained physicians (T.T., J.U., A.H., Y.F., Y.O., S.F., T.M., and M.E.) at weeks 0, 4, 8, and 52 using the CAI [13]. The endoscopic disease activity was assessed at weeks 0, 4, and 52 based on the MES [14] by experienced endoscopists who specialize in inflammatory bowel disease (Y.M., T.T., J.U., A.H., Y.F., Y.O., S.F., T.M., and M.E.). The histological disease activity was assessed using the Geboes score (GS) [15]. Each rectal biopsy sample was assessed by pathologists (S.K., Y.O., and Y.O.) at weeks 0, 4, and 52.
Medical interviews and blood tests were performed at each clinical visit, and the results were analyzed by trained physicians to determine AEs related to IN. In the middle of the study period, the possible association of IN with pulmonary arterial hypertension (PAH) [16] was suspected, and medical interviews concerning breathlessness and echocardiogram at weeks 0, 4, and 52 were added thereafter.
3. Data Collection and Definitions
Clinical information for each patient was determined at study entry and was classified based on the Montreal classification [17].
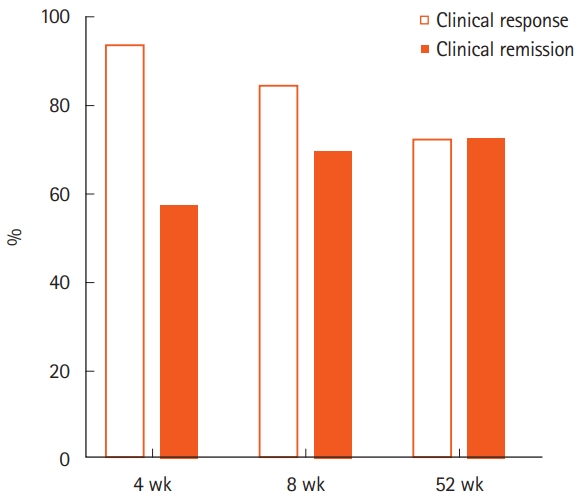
At each assessment, clinical response was defined as a decrease in the CAI score of at least 30% from baseline. Clinical remission was defined as CAI Ōēż 4. Mucosal healing was defined as MES Ōēż 1, and complete mucosal healing was defined as MES = 0. Histological healing was defined as GS Ōēż 1.
AEs were classified as mild or severe. Severe types included AEs that required hospitalization, while mild types included those not requiring hospitalization. For blood test abnormalities, liver dysfunction was defined as a serum transaminase level that was greater than twice the upper normal limit. Renal dysfunction was defined as the decrease of the estimated glomerular filtration rate by Ōēź 30% from the baseline level. We regarded colitis with markedly edematous changes that were recovered only by the discontinuation of IN as an AE.
4. Biopsy Sampling
Mucosal biopsy samples were collected at weeks 0 and 52 during colonoscopy. For each colonoscopy, patients were prepared using standard bowel cleaning with 2 L of lavage solution (Niflec┬«; EA Pharma Co., Tokyo, Japan). Mucosal biopsy samples were obtained from the rectum using disposable biopsy forceps (Olympus, Tokyo, Japan) after washing the rectal mucosa gently with tap water containing a dimethicone solution. Biopsy samples were immediately frozen at ŌłÆ80┬░C until extraction of microbial DNA.
5. DNA Extraction, Sequencing, and Processing of 16S Ribosomal RNA Gene
Mucosal microbial DNA was extracted as previously described with minor modification [18,19]. The V4 region of the 16S ribosomal RNA gene was amplified by polymerase chain reaction using the primers 515F/806R, which included the Illumina flow cell adapter sequence and a unique 12-base barcode sequence. Subsequently, multiplexed 16S amplicon sequencing was performed on the MiSeq Illumina platform (Illumina Inc., San Diego, CA, USA). Detailed methods are described in the Supplementary Material. The sequences were analyzed using QIIME version 1.9.1 software [20], which is available at http://www.qiime.org.
6. Statistical Analysis
Categorical variables were described using frequencies and percentages, and continuous variables were described using medians and interquartile ranges (IQRs). Clinical response and remission rates were calculated using non-responder imputation, where dropouts were assumed to be non-responders regardless of their actual disease activity at the time of dropout. The mucosal healing and histological healing rates were calculated using non-responder imputation. Changes in CAI, MES, C-reactive protein (CRP), and GS were estimated by the Wilcoxon signed-rank test. P-values were considered to be statistically significant at a level of < 0.05.
7. Ethical Considerations
This study protocol was approved by the Institutional Review Board at Kyushu University in compliance with the Declaration of Helsinki Principles (registration number: 27067). All patients enrolled in this study received and reviewed the study information, and then voluntarily provided written informed consent upon participation. This study was registered at the University Hospital Medical Information Network Center (UMIN Clinical Trials Registry, number UMIN 000022575).
RESULTS
1. PatientsŌĆÖ Characteristics
We offered 36 patients, and 2 patients declined to participate, a patient did not meet the inclusion criteria. Thirty-three patients with UC were enrolled in the present study (Supplementary Fig. 1). The baseline characteristics of the patients are shown in Table 1. The median age was 29 years (IQR, 23-48 years) and the median disease duration was 3 years (IQR, 1-8 years). The left-sided type was present in 5 patients and the extensive type was present in 28 patients. The median CAI score, serum CRP level, and MES at baseline were 8 (IQR, 8-11), 3.0 mg/L (IQR, 1.4-8.9 mg/L), and 2 (IQR, 2-3), respectively.
The main reasons for the induction of IN were as follows. Four patients were steroid refractory. There were 12 steroid dependent patients, 10 of whom were on oral prednisolone (PSL) while tapering off and 2 were relapsed and entered this study after discontinuation of PSL. PSL was being administered to 14 patients at study enrolment. Primary non-responder to anti-tumor necrosis factor (TNF)-╬▒ agents were 7 patients, secondary failure to anti-TNF-╬▒ agents were 5 patients. These 12 patients had been continuously treated with anti-TNF-╬▒ agent therapy for more than 8 weeks prior to study enrolment. Two patients were relapsed after cessation of tacrolimus, and 1 patient had insufficient response to cyclosporine. There were 2 patients with no induction therapy other than IN. Concurrent medicines were shown in Table 1. No patient was newly started on a drug other than IN as induction therapy.
2. Clinical Efficacy of IN as Induction and Maintenance Therapies
The clinical response rates at weeks 4, 8, and 52 were 93.9% (31/33), 84.8% (28/33), and 72.7% (24/33), and the clinical remission rates at each assessment were 57.6% (19/33), 69.7% (23/33), and 72.7% (24/33), respectively (Fig. 1). The trends for CAI were described in Supplementary Fig. 2, and the details of the clinical courses were as follows. Among 33 patients, 2 were primary non-responders to IN and 1 discontinued IN because of an AE. Six patients discontinued IN during follow-up because of a loss of response to IN in 3, unwillingness to continue the study in 2, and AEs in 1 patient. The remaining 24 patients maintained clinical remission at week 52 (Supplementary Fig. 1). All of the 24 patients showed clinical response at week 4. Of the 24 patients, 79% (19/24) achieved clinical remission within 8 weeks and the remaining 21% after 8 weeks (Fig. 2).
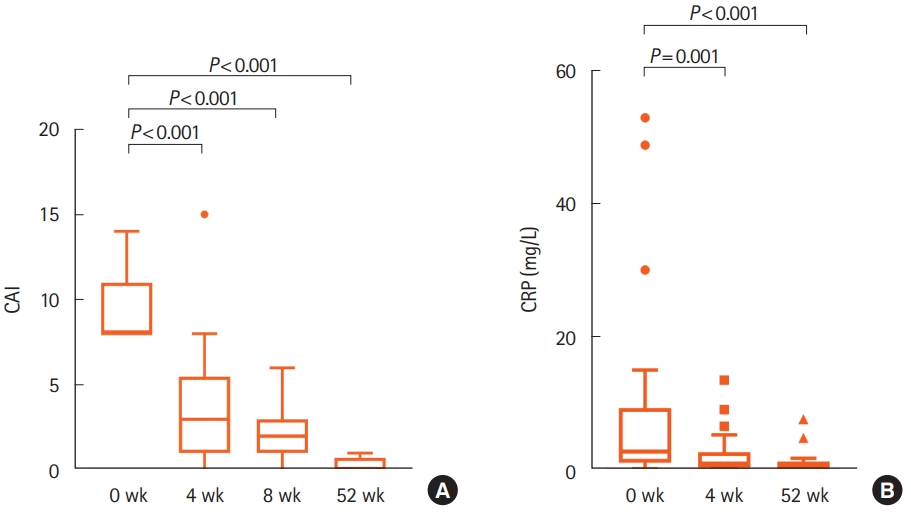
Fig. 3 shows the trends for CAI and CRP scores. The median CAI score was significantly lower at weeks 4, 8, and 52 than before the administration of IN (P<0.001, P<0.001, P<0.001, respectively). The median CRP score was also significantly lower at weeks 4 and 52 than before the administration of IN (P= 0.001, P< 0.001, respectively).
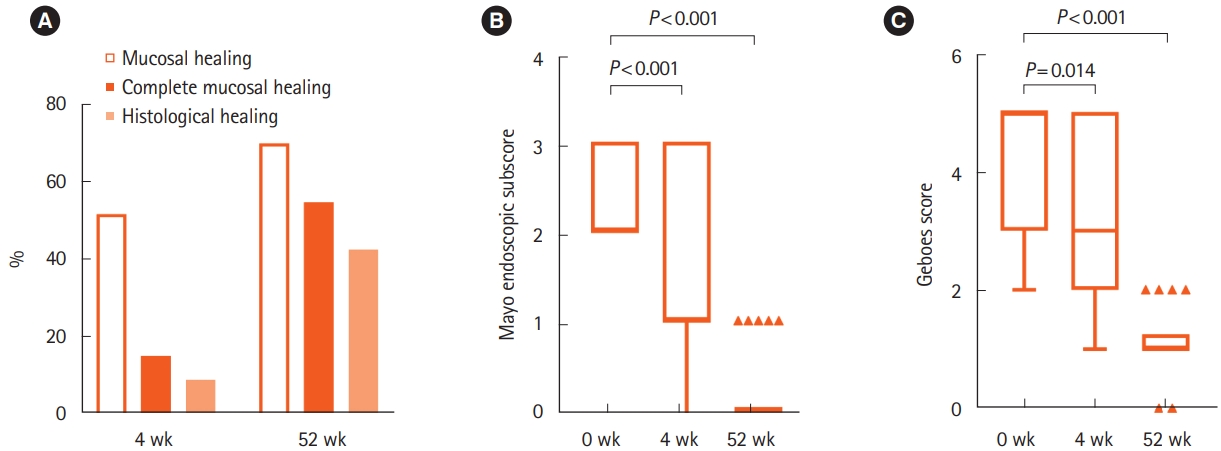
Endoscopic assessment was performed in 32 patients at week 4 and 24 patients at week 52. The mucosal healing rates at each assessment were 51.5% (17/33) and 69.7% (23/33), respectively. The complete mucosal healing rates at weeks 4 and 52 were 15.2% (5/33) and 54.5% (18/33), respectively (Fig. 4A). The median MES was significantly lower at weeks 4 and 52 than before the administration of IN (P< 0.001, P< 0.001, respectively) (Fig. 4B). Histological disease activity was assessed in 28 patients at week 4 and 18 patients at week 52. The median GS was also significantly lower at weeks 4 and 52 than before the administration of IN (P= 0.014, P< 0.001, respectively) (Fig. 4C).
Among 14 patients with concurrent PSL at baseline, 8 patients were achieved clinical remission with IN therapy at week 52 and were able to discontinue PSL. Regarding other concurrent therapy, anti-TNF-╬▒ agents were discontinued in 5 (5/12, 41.7%) and thiopurine were stopped in 3 patients (3/18, 16.7%), and remission was maintained with IN treatment during follow-up period.
3. Safety Assessment
Twenty-four AEs were reported in 17 patients during the study period (Table 2). Among them, 19 AEs (headache, liver dysfunction, mild epigastric pain/abdominal pain, and renal dysfunction) in 15 patients were considered mild, and 7 AEs (acute colitis, intussusception, infectious colitis, portal thrombosis, and appendicitis) in 4 patients were considered severe.
All mild AEs except for renal dysfunction occurred relatively early after induction therapy with IN and were reversible. However, a dose reduction of IN was required to improve abdominal pain in 1 patient and liver dysfunction in 2 patients. The other patients continued IN at a dose of 2 g/day, and the AEs were resolved without additional therapeutic intervention. Renal dysfunction was found in 1 patient treated concurrently with an anti-TNF-╬▒ agent. The estimated glomerular filtration rate of this patient gradually decreased from 72.4 mL/min/1.73 m2 at baseline to 49.6 mL/min/1.73 m2 at week 52.
Severe AEs were reported in 4 patients. Acute colitis developed in 3 patients, of whom 1 developed complicated intussusception. Three patients manifested acute severe abdominal pain and computed tomography showed marked colonic wall edema, as previously described [21-23]. However, 1 patient developed acute colitis 8 months later, with complications that reportedly occurred within 3 months after the induction of IN [11]. Another patient subsequently developed acute appendicitis after the improvement of colitis and required surgery. The remaining patient with infectious colitis caused by Clostridium perfringens simultaneously developed portal vein thrombosis. No patient showed complications related to PAH during follow-up.
4. Comparison of Microbial Composition before and after IN Treatment
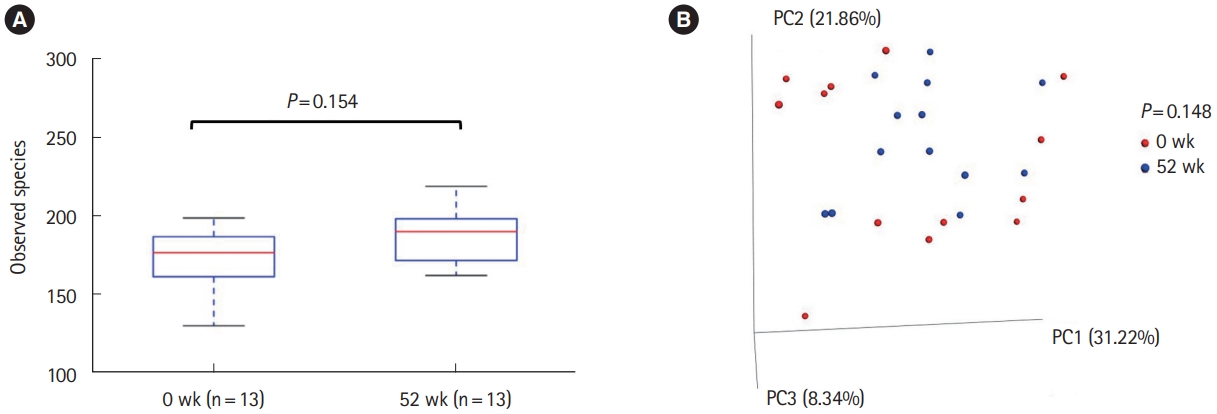
The microbial composition was compared before and after IN treatment in 21 of 24 patients who achieved clinical remission at week 52. Additionally, 1,616,663 reads were obtained after quality control with a mean 62,179 reads per sample. Eight patients were excluded from the analysis because the number of reads from their samples were too small ( < 5,000). Consequently, the differences in microbial composition before and after IN were compared in 13 patients. The alpha diversity by the observed species index was not significantly different before and after IN treatment (P= 0.154) (Fig. 5A). The beta diversity by the metrics of weighted UniFrac also did not differ significantly (P= 0.148) (Fig. 5B). We subsequently compared the taxonomic composition before and after IN treatment. The abundance of genera Ruminococcus, Dorea, Actinomyces, Oribacterium, Eubacterium, Clostridium, and Finegoldia, the family Caulobacteraceae, and the order Streptophyta were significantly greater, and the abundance of genus Pediococcus was significantly lower, in mucosal samples after IN compared with those before IN (Supplementary Fig. 3). However, no significant difference was observed in the abundance of the Bacteroides and Bifidobacterium families, in contrast to a previous report [10].
DISCUSSION
Although IN as induction therapy for UC has shown favorable clinical efficacy, its maintenance effect remains uncertain. As for the induction therapy, the present study also showed that the clinical response rates at 8 weeks were 84.8%. The subjects were all different from the participants in previous retrospective study [11], yet they showed similar efficacy at 8 weeks. Several studies also reported the usefulness of IN as induction therapy in active UC [9-11]. As for the maintenance therapy, our prospective study showed the clinical response rate and remission rate at week 52 was 72.7%, indicating the high efficacy of IN as long-term effect as well.
Regardless of the efficacy shown by IN, there are some safety concerns [9,10,24]. A recent Japanese nationwide survey reported that mild AEs related to IN included liver dysfunction, gastrointestinal symptoms, and headache, and these occurred in 4.6%, 2.4%, and 1.5% of patients, respectively [25]. Our study revealed that mild AEs related to IN occurred at a much higher rate. These mild AEs could be missed due to the degree of physician awareness, therefore, physicians should be aware that mild AEs occur more frequently than reported previously. Additionally, most mild AEs were resolved only when the IN dose was reduced.
In the present study, 7 severe AEs that require hospitalization occurred in 4 patients, and acute colitis was the most frequent severe AE (9%). Based on the Japanese nationwide survey, the risk of colonic intussusception and colitis were 1.1% and 0.9%, respectively [25]. Acute colitis caused by IN was characterized by the acute onset of colicky abdominal pain and endoscopically severe edematous mucosa without mucosal defects, which is distinct from flare-up of UC [21-23]. This complication was reported to occur within 8 weeks after induction therapy with IN, and occasionally develops into colonic intussusception [21,23]. Although portal vein thrombosis was founded in the present study, dehydration caused by infectious colitis also occurred, which may be indirect AE of IN. The most alarming AE reported in the past was PAH [25]. PAH was not observed in the present study, probably because PAH was rare AE. It is controversial whether PAH caused by IN can recover after the discontinuation of IN or not [26,27], therefore, physicians should carefully consider PAH during the administration of IN.
The optimal IN dose to induce remission remains undetermined. A recent randomized controlled trial (RCT) showed a significant dose-dependent linear trend in the clinical response at week 8, but 2.0 g/day of IN had no advantage for clinical remission and mucosal healing compared with 1.0 g/day of IN [10]. Because the results of the RCT had not been published at the beginning of the present study, we started IN at a dose of 2.0 g/day as induction therapy. Considering that most AEs were resolved after dose reduction in the present study, optimal dose with further reduction needs to be clarified.
In the present study, the possible influence of IN on colonic microbial composition was assessed using mucosal biopsy samples at 52 weeks. AhR signaling, the main mechanistic pathway that mediates the effects of IN, was reported to modulate host-microbiota communication [7,8]. Additionally, Naganuma et al. [10] demonstrated that IN might partly modify colonic microbiota composition using fecal samples at 8 weeks. However, we did not find a significant influence of IN on colonic microbial diversity. The modifying effect of IN on colonic microbial diversity plays may change with long-term time.
Our study had some limitations. First, this study was an uncontrolled open-label study without a placebo group. Because a high placebo effect in UC is well known,28 an RCT will provide more reliable results to determine the true clinical efficacy of IN. Second, this study was performed at a single center with a limited number of patients. However, we think that the present study will have some clinical impact because this was the first prospective study to analyze the efficacy of IN in maintaining remission in patients with UC.
In conclusion, IN might be a therapeutic option to induce and maintain remission in moderate to severe UC, although the relatively high rate of AEs should be considered. Further studies are required to determine the appropriate dose to induce and maintain remission and to evaluate the safety concerns related to IN for refractory UC.