INTRODUCTION
Acute severe ulcerative colitis (ASUC) is a severe flare of ulcerative colitis (UC) that affects approximately 25% of patients with UC at some point in their lives [1]. It is defined by the Truelove and Witts criteria as 6 or more bowel actions per day with blood, along with at least one of the following: pulse rate > 90 beats/min, temperature > 37.8°C, hemoglobin < 10.5 g/dL, and erythrocyte sedimentation rate > 30 mm/hr [2].
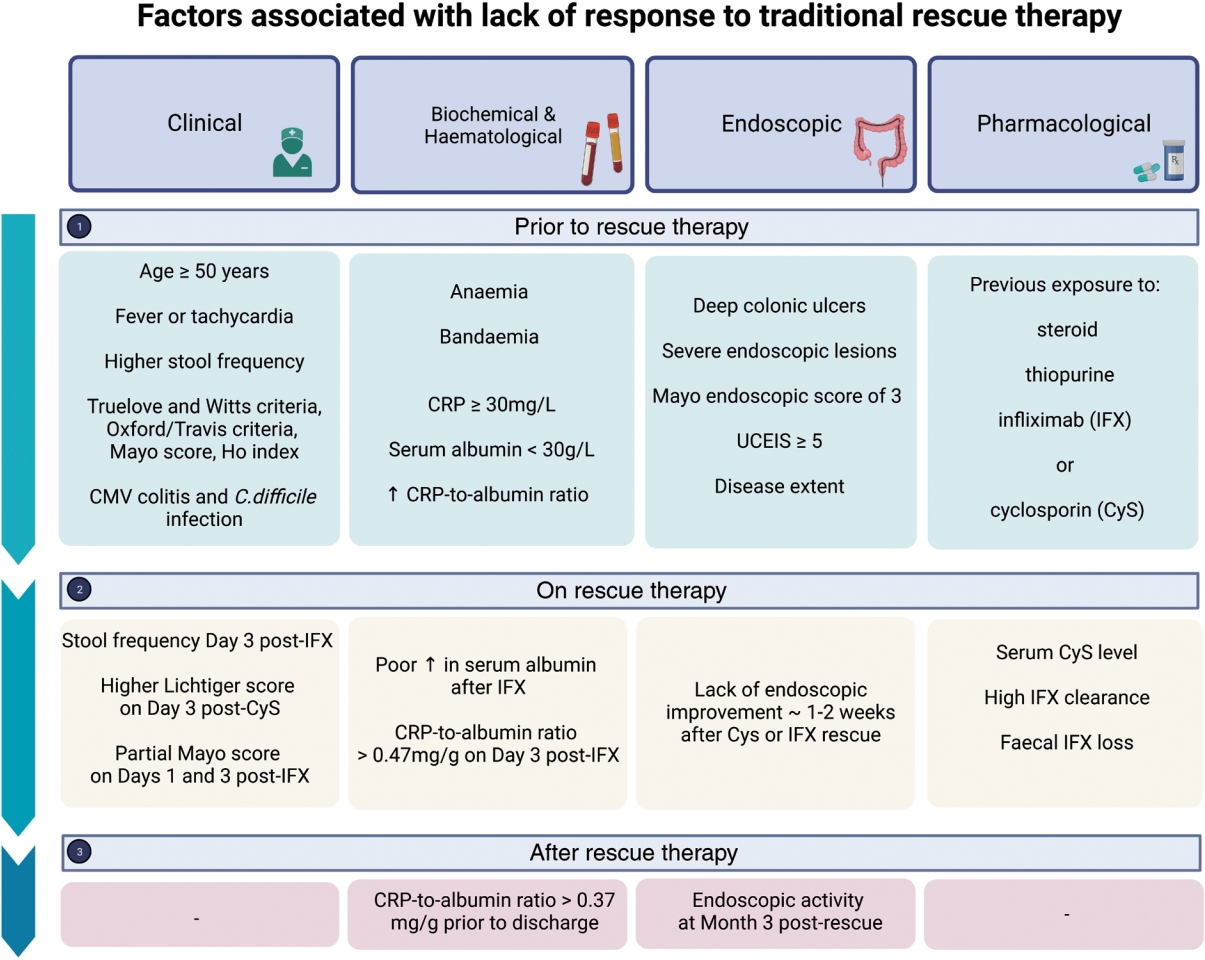
Approximately 30% of patients are refractory to intravenous (IV) steroids and require rescue therapy with either infliximab or cyclosporin [3,4]. Approximately 50% of patients respond to infliximab or cyclosporin [3,5,6]. Patients who fail rescue therapy face the prospect of emergency colectomy. Poor prognostic factors associated with lack of response to traditional rescue therapy have been recently identified [7] and are summarized in Fig. 1.
Emerging data suggests that clinical outcomes of steroid-refractory ASUC may be improved with novel infliximab dosing strategies, use of cyclosporin as a bridge to slower acting biologic agents and Janus kinase (JAK) inhibitors as sequential therapy [8-11]. In this review, we provide an overview of the traditional rescue therapies available in ASUC and mechanisms of failure of rescue therapies. We then summarize and synthesize the emerging literature on contemporary approaches to clinical management of ASUC in the setting of failure to respond to traditional rescue therapies.
SEARCH STRATEGY
References for this review were identified through electronic searches of Ovid Medline and EMBASE (inception to December 2023), and conference proceedings identified using EMBASE (January 2020 to December 2023). The following search terms were used alone or in combination: “acute severe colitis,” “ASUC,” “ulcerative colitis,” “hospital,” “severe,” “infliximab,” “cyclosporin,” “ciclosporin,” “tofacitinib,” “upadacitinib,” “vedolizumab”, or “ustekinumab.” Only papers published in English were reviewed. The final reference list was generated based on originality and relevance to the scope of this review.
EXISTING RESCUE THERAPIES FOR ASUC
Therapies in ASUC require a rapid onset of action to target the aberrant immune response. Patients with ASUC who fail first-line therapy with steroids need rescue therapy with either infliximab or cyclosporin, both of which are equally effective based on data from 2 randomized controlled trials [5,12]. A meta-analysis of non-randomized studies indicated that infliximab was associated with better clinical response, odds ratio (OR) 2.96 (95% confidence interval [CI], 2.12-4.12) and lower 12 months colectomy rates, OR 0.42 (95% CI, 0.22-1.28) [6]. Regardless of these findings the clinical response and early colectomy rates have been similar between the 2 drugs. Long-term response rates have also remained similar; albeit with higher relapse rates in cyclosporin compared with infliximab-treated patients [3].
1. Cyclosporin
Cyclosporin exerts its action by binding to the cytoplasmic protein cyclophilin, thereby inhibiting calcineurin, a regulatory factor. This in turn inhibits the production of multiple cytokines including interleukin (IL)-2, IL-3, IL-4, tumor necrosis factor (TNF)-α, interferon-gamma and granulocyte-macrophage colony-stimulating factor, thereby inhibiting T-cell proliferation and differentiation [13].
1) Short-term Efficacy
In clinical trials, cyclosporin has been shown to have immediate response rates at 1 to 2 weeks between 64% and 82% [14,15] and colectomy rates at 3 months have ranged from 26% to 47% [5,12,14-16]. Rates of short-term clinical response, 3 months after cyclosporin have been between 40% and 54% [5,12,16].
4) Dosing Schedule
Cyclosporin is administered as a continuous IV infusion for 7 days, following which patients are transitioned to oral cyclosporin. Given the lack of difference found in short-term colectomy rates, median time to response and side effects between patients receiving 2 and 4 mg/kg/day [19], current guidelines suggest 2 mg/kg/day along with therapeutic drug monitoring to minimize the risk of long-term cyclosporin toxicity [20]. Although the optimal duration of therapy is unknown, it is often limited to 3 months to minimize the risk of adverse events.
2. Infliximab
Infliximab is a monoclonal antibody that binds to TNF-α, preventing its interaction with TNF receptors, thereby inhibiting downstream inflammatory activity [21]. Infliximab also enhances apoptosis of activated effector lymphocytes and restores the number of T-regulatory cells in the mucosa [22-24].
3) Safety Profile
Infliximab has a good safety profile in ASUC; however, it is contraindicated in untreated tuberculosis, demyelinating disease, congestive cardiac failure (New York Heart Association Class iii or IV) and active infection [29].
4) Dosing Schedule
The traditional administration schedule of infliximab has been three 5 mg/kg doses at weeks 0, 2, and 6. However, in clinical practice, dose-escalated infliximab rescue strategies are often employed in an effort to improve response rates. Dose-escalated infliximab rescue strategies include an accelerated schedule whereby patients may receive three 5 mg/kg doses in a shorter time frame (e.g., within 3 weeks) and an intensified dosing schedule whereby patients are administered higher infliximab doses (e.g., 10 mg/kg doses).
The optimal infliximab dosing regimen in ASUC is unknown. A meta-analysis concluded that infliximab dose intensification with either accelerated or high-dose induction strategies did not reduce 3-month colectomy rates compared to standard induction (OR, 0.70; 95% CI, 0.39-1.27; P= 0.24) [9]. However, patients with more severe disease (higher C-reactive protein and lower albumin) were more likely to have received dose-escalated infliximab, thereby potentially confounding the results. Randomized controlled trial data are therefore required to help inform the optimal infliximab dosing strategy in ASUC. Trials exploring a pharmacokinetics driven dashboard model of infliximab dosing versus standard care (NCT03937609) and intensified versus standard infliximab dosing (NCT02770040) strategy are currently under way.
CHALLENGES IN SELECTING THE RIGHT RESCUE THERAPY IN ASUC
Whilst infliximab and cyclosporin are considered equally effective as rescue therapy in steroid-refractory ASUC, selecting the right rescue therapy in ASUC can be challenging and should be individualized based on patient factors, the presence of comorbidities, the intended choice of maintenance therapy after successful induction of remission, and physician and local hospital familiarity with the rescue therapy of choice.
1. When to Consider Infliximab as Rescue Therapy
Infliximab is preferred by many clinicians in view of its ease of administration [30,31]. It also enables the administration of dose-escalated doses (higher or additional doses) although there is insufficient evidence to support such practice.
Infliximab should be considered preferentially in patients in whom cyclosporin is contraindicated (e.g., the presence of renal impairment) and where the risk of nephrotoxicity is high (e.g., concomitant nephrotoxic drug use). Given the narrow therapeutic window of cyclosporin, infliximab is also preferred in settings where cyclosporin therapeutic drug monitoring is unavailable.
While most patients presenting with ASUC have either a known history of UC or typical findings of UC at endoscopy, in some patients the diagnosis is less clear raising the possibility of an acute severe presentation of Crohn’s disease. In the setting of diagnostic uncertainty, infliximab is the preferred rescue therapy given the wider body of evidence supporting infliximab’s use in both UC and Crohn’s disease.
2. When to Consider Cyclosporin as Rescue Therapy
Cyclosporin should be considered as first-line rescue therapy in patients who are thiopurine naïve and those with contraindications to infliximab including the presence of demyelinating conditions such as multiple sclerosis and moderate to severe heart failure.
3. How Anticipated Maintenance Therapy May Influence Choice of Rescue Therapy
Although successful induction of remission is the primary focus when faced with a patient with ASUC, anticipating the choice of maintenance therapy after successful of remission may also guide the choice of rescue therapy. As a monoclonal antibody, infliximab is at risk of immunogenicity which involves the development of antibody formation to infliximab itself. The highest risk of immunogenicity occurs during periods of low trough infliximab levels which tends to occur following initial infliximab dose administration due to increased infliximab clearance and in patients in whom infliximab is used solely as a rescue agent without its continuation as a maintenance therapy [32]. Periods of low infliximab levels increase the potential for pseudo-episodic exposure to infliximab, which increases the likelihood of antibody formation and risk of infliximab failure should it be required as a therapy in the future. Similarly, patients who go on to receive maintenance infliximab monotherapy may also be at increased risk of immunogenicity [33].
There has been growing interest in the use of cyclosporin as an induction regimen followed by maintenance with a slower acting agent such as vedolizumab or ustekinumab, both of which carry a lower risk of immunogenicity [34]. Cyclosporin induction with vedolizumab or ustekinumab as maintenance may be employed in patients with a history of severe infections or active malignancy for whom prolonged systemic immunosuppression with infliximab may not be desirable. Such “bridging” approaches are discussed further in the maintenance section of this article.
Overall, in patients in whom infliximab maintenance therapy is anticipated, infliximab induction is preferred. In contrast, in patients in whom an alternative biologic is anticipated as maintenance therapy, cyclosporin induction may be preferable.
MECHANISMS OF INFLIXIMAB FAILURE
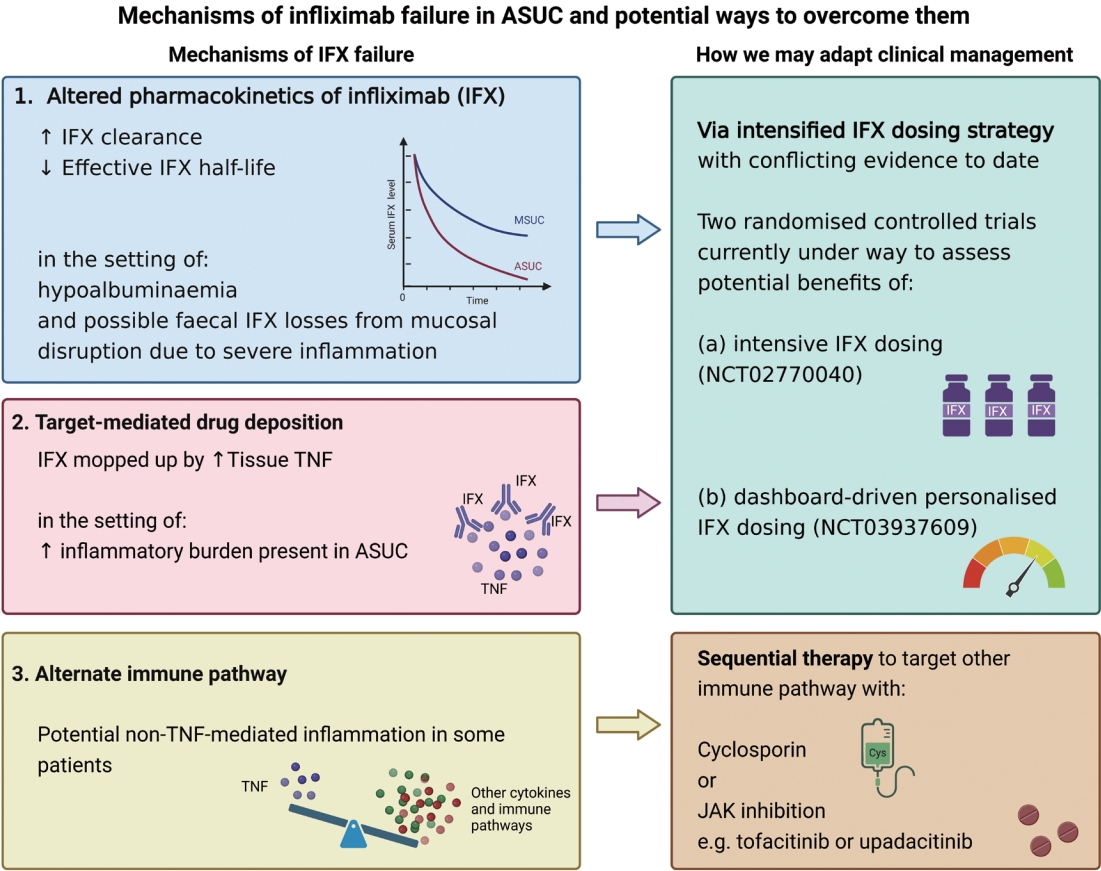
Three main mechanisms of infliximab failure have been postulated in ASUC: (1) altered pharmacokinetics of infliximab in ASUC; (2) high TNF burden in ASUC leading to target-mediated drug deposition; and (3) alternate (non-TNF-mediated) immune pathways in some patients [35]. Fig. 2 provides a summary of the mechanisms of infliximab failure and how clinical management may be adapted.
1. Altered Pharmacokinetics of Infliximab
Infliximab clearance is considered to be the biggest driver of therapeutic outcomes in ASUC [35].
Whilst a definite dose-exposure relationship for infliximab in ASUC is yet to be established, 2 studies have examined the relationship between infliximab clearance and outcomes [32,36]. In a pharmacokinetic study of 36 patients with corticosteroid-refractory UC who received infliximab, infliximab responders at week 14 had a longer effective infliximab half-life (P= 0.005) and reduced clearance (P= 0.002) compared to non-responders [32].
Similarly, in a recent study of 39 patients with ASUC where infliximab clearance was calculated based on an existing formula, patients who required colectomy at 6 months had a higher median infliximab clearance compared to those who avoided colectomy (0.733 L/day vs. 0.569 L/day, P= 0.005). Patients with a calculated clearance above 0.627 L/day were more likely to require colectomy at 6 months compared to those with lower clearance (61.5% vs. 7.7%, P= 0.001). Baseline infliximab clearance was the only factor associated with colectomy on multivariable logistic regression [36].
Factors known to influence clearance include serum albumin level, sex and the presence of anti-drug antibodies [37]. As an acute phase reactant of inflammation, hypoalbuminemia is often observed in patients with more severe disease, thus contributing to the higher infliximab drug clearance in such patients.
Disruption of the intestinal barrier in the setting of inflammation has also been proposed as a factor contributing to increased drug clearance [35]. In ASUC, patients with more severe disease often exhibit severe mucosal lesions characterised by deep or large ulcers. Whilst no direct correlation has yet been found between the severity of endoscopic findings and fecal infliximab loss in the stool [38], it remains plausible that endoscopic severity may contribute to increased gut permeability, and in turn result in increased fecal infliximab loss.
While increased infliximab clearance has been linked to poorer outcomes in ASUC, it is currently unclear whether increased clearance can be overcome via more intensive infliximab dosing (NCT02770040) or dashboard-driven infliximab dosing (NCT03937609).
2. Target-Mediated Drug Deposition
Target-mediated drug disposition (TMDD) is another major mechanism implicated in infliximab failure in ASUC. TMDD refers to a phenomenon where a drug has a high affinity to a pharmacological target, leading to significant drug binding to the target, thereby affecting the pharmacokinetic properties of the drug [39].
Tissue TNF levels have been shown to correlate with disease activity in inflammatory bowel disease with patients with more severe disease having higher levels of TNF in the intestinal mucosa [40,41]. As a monoclonal antibody, infliximab has a high affinity for TNF. High levels of TNF in the setting of severe inflammation have been likened to a “sponge” that rapidly binds to or mops up infliximab molecules [35], resulting in increased infliximab clearance.
In a study of patients with Crohn’s disease and UC, patients with active inflammation had a higher TNF to anti-TNF ratio in tissue compared to uninflamed tissue [40]. While this study did not directly examine TMDD, it provides a potential mechanistic explanation for infliximab failure in patients with ASUC who have a high inflammatory burden.
Higher infliximab dosing may be able to overcome the high TNF burden and increased TMDD observed in some patients. Controlled data supporting this approach are however currently lacking and is the subject of ongoing research (NCT02770040 and NCT03937609).
3. Alternate Immune Pathways
Whilst TNF-α blockade has been the mainstay of ASUC management, a significant proportion of patients still however do not respond to standard or dose-intensified infliximab. This hints to a potential alternate, non-TNF-mediated pathway being predominantly activated in some patients. This hypothesis is supported by studies where cyclosporin, tofacitinib, and upadacitinib have been successful in inducing remission in some patients who had previously not responded to infliximab [10,11,34,42-50].
MECHANISMS OF CYCLOSPORIN FAILURE IN ASUC
Data on mechanisms of cyclosporin failure in ASUC are limited. Multidrug resistance gene-1 (MDR1) encodes for the transporter P-glycoprotein, a plasma membrane protein involved in the transport of cyclosporin out of the cell into the gut lumen [51]. In ASUC patients receiving cyclosporin, Daniel et al. [51] observed significant differences in MDR1 between responders and non-responders.
Other potential reasons for cyclosporin failure may relate to the high interindividual variability in cyclosporin metabolism and pharmacokinetics, which can in turn be partly explained by genetic polymorphisms. Cyclosporin is predominantly metabolized by cytochrome P450 3A4 (CYP3A4) in the liver and small bowel [52], and primarily excreted by the biliary system [53]. As such, inter-patient differences in metabolism via the CYP3A4 system may affect cyclosporin levels and/or dosing requirements [54]. Similarly, concomitant use of drugs, such as phenytoin and carbamazepine, that induce CYP3A4 may contribute to subtherapeutic cyclosporin levels [55] and potentially contribute to higher rates of non-response.
In view of the hepatic metabolism of cyclosporin, patients with advanced chronic liver disease may be at increased risk of supratherapeutic cyclosporin levels [56] and therefore require closer monitoring of blood cyclosporin levels and dose titration.
SEQUENTIAL THERAPY
Sequential therapy refers to the use of a second rescue agent after failure of a first rescue agent in a bid to induce remission and avoid emergency colectomy.
1. Sequential Therapy with Infliximab or Calcineurin inhibition
1) Short-term Response Rate
In a systematic review of 314 patients who received infliximab after non-response to calcineurin inhibition (cyclosporin/tacrolimus), or vice-versa, sequential therapy was associated with an overall immediate clinical response rate of 62.4% (95% CI, 57.0%-67.8%), clinical remission rate of 38.9% (95% CI, 33.5%-44.3%), colectomy rate at 3 months of 28.3% (95% CI, 21.7%-34.5%) and 12 months of 42.3% (95% CI, 36.0%-48.6%) [57]. Overall, clinical outcomes including response rates, colectomy rates, adverse events and the risk of infection appeared similar irrespective of whether infliximab or a calcineurin inhibitor was used as the first agent [57]. While 3 deaths occurred in the 252 patients who received infliximab sequential therapy after failure of calcineurin inhibition, compared to no deaths in the 62 patients who received a calcineurin inhibitor after infliximab failure, conclusions on comparative safety cannot be drawn due to the small number of patients who received the latter regimen [57].
2) Long-term Response Rate
A significant proportion of patients went on to require colectomy at 3 and 12 months (30.0% and 56.7%, respectively) [57].
3) Safety Profile
The rate of adverse events was 23.0% (95% CI, 17.7%-28.3%); serious infections, 6.7%; and, mortality, 1% [57]. The risk of sequential therapy is lower than originally reported but is a strategy that is best reserved for selected patients in specialist centers familiar with calcineurin inhibition with close monitoring and engagement of the multidisciplinary team.
2. Tofacitinib Use after Biologic Failure
More recently, tofacitinib has been used as a sequential therapy in ASUC predominantly after failure of one or more biologics, or as first-line rescue in biologic-experienced patients presenting with ASUC [10,42,44-48,58-69]. These studies are summarized in Table 1. Tofacitinib works by inhibiting intracellular JAK (predominantly JAK 1 and 3, and to a lesser extent JAK 2) and subsequent phosphorylation of signal transducers and activators of transcription, causing decreased production of multiple cytokines [70]. This in turn leads to a decreased differentiation of naïve T helper cells into the Th1, Th2, and Th17 cells [71].
1) Short-term Response
In a review of 14 studies involving 134 patients, most of whom had failed one or more biologics, the overall response rate (with avoidance of colectomy) was 77% (95% CI, 70%-85%) [34]. In a subset of these patients (n = 55) from a GETAID-TALC (the largest of the cohorts), of whom 49 had failed infliximab previously and 19 had previously been exposed to cyclosporin, at week 6, 33 out of 55 (60%) had clinically responded, 25 out of 55 (45.5%) achieved clinical remission and 20 out of 55 (37.5%) achieved clinical steroid-free remission [44]. In the latter study, at week 14, 23 out of 55 (41.8%) had clinically responded, 19 out of 55 (34.5%) achieved clinical remission and 18 out of 55 (32.7%) achieved clinical steroid-free remission. Colectomy-free survival at 3 months was 78.9% [44].
2) Long-term Response
A theoretical advantage of tofacitinib is the ability to continue it as maintenance once remission has been achieved; however, long-term data are limited and some patients may experience a loss of efficacy over time. In the GETAID-TALC study of 55 patients colectomy-free survival at 6 months was 73.6% [44]. Of the 3 other small series with long-term outcomes response rates are variable; in one study 2 out of 5 initial responders to tofacitinib required IV steroids at 6 months [47]; in a second study 2 out of 5 patients who initially avoided colectomy required colectomy by week 26 [48] and in the third series of those who initially responded to tofacitinib all remained colectomy free out to 12 months [46].
3) Safety Profile
In a review of 14 studies of tofacitinib in ASUC the overall serious adverse rate was 3.3% with no mortality directly attributable to tofacitinib [34]. Nonetheless among the 2 patients who were exposed to tofacitinib as sequential therapy one death was in a patient with COVID-19 and probable pulmonary embolus [63] while the second death was in an 81-year-old man with chronic obstructive airways disease and concomitant diabetes mellitus who had a delayed colectomy [44].
4) Dosing
The tofacitinib dosing applied to ASUC has varied in total dose and duration and has generally comprised 10 mg BD (twice a day) or 10 mg TDS (three times a day) induction dosing, with the total duration of the TDS dosing varying from 2 days to 2 weeks.
These preliminary data suggest that tofacitinib is a promising rescue therapy for ASUC. However, further data are required regarding tofacitinib’s safety, efficacy and durability of response which may be informed by 2 prospective open-label studies (NCT04925973 and NCT05112263).
3. Upadacitinib Use after Biologic Failure
Upadacitinib, a newer JAK inhibitor, has a more pronounced inhibitory effect on JAK1 compared to JAK 2, JAK 3, and TYK2 [72]. The relationship between inhibition of specific JAKs and treatment response in ASUC is however unknown. Data regarding upadacitinib are limited to case studies and case series [11,49,50,73].
1) Short-term Response
In an Australian study by Gilmore et al. [49] of 6 patients, all of whom had been previously exposed to infliximab prior to admission (3 with primary non-response; 2 with secondary loss of response, and 1 who was intolerant), upadacitinib 45 mg daily was commenced for 16 weeks after failure to respond to 3 days of IV hydrocortisone. Five of 6 patients achieved colectomy-free survival at 30 days. In a study from Israel of 4 patients who had failed IV steroids and infliximab, upadacitinib 45 mg orally daily was commenced. Three of 4 patients achieved clinical response within 4 to 8 days and 1 of 4 patients underwent colectomy within 3 weeks. Three of 4 patients demonstrated colectomy-free survival at 4 months [11]. In a separate study by Berinstein et al. [50], (presented in abstract form) of 13 patients comprised of 10 patients with UC and 3 with Crohn’s disease, high-dose upadacitinib 30 mg orally BD was used for 1 week. More than half (61.5%) avoided bowel surgery.
2) Long-term Response
A single case report has indicated colectomy-free survival out to 6 months in a patient previously exposed to azathioprine, infliximab, adalimumab, and tofacitinib [73].
3) Safety Profile
In the study of 6 patients by Gilmore et al. [49] with patients exposed to infliximab prior to admission 2 patients experienced acne. In the study by Berinstein et al. [50] exploring high-dose upadacitinib severe adverse events included: 1 case of venous thromboembolism and several infections; (1) COVID-19; (2) bacteremia; (3) cytomegalovirus; (4) Nocardia; (5) 2 post-surgical infections. There were no severe adverse events and no cardiovascular or thrombo-embolic events in the remaining case series to date [11,49,73].
4) Dosing
The dosing applied to ASUC has varied in total dose and duration and comprise both 30 mg BD and 45 mg daily with total duration varying from 3 days to 60 days respectively.
Taken together these data suggest that upadacitinib may be a feasible rescue therapy in those previously exposed to anti-TNF prior to or during their admission for ASUC. However, randomized controlled data are required to establish the optimal dose, duration of therapy and safety and efficacy profile of upadacitinib in ASUC.
MAINTENANCE THERAPY FOLLOWING SUCCESSFUL INDUCTION OF REMISSION IN ASUC
At present, the evidence supporting maintenance therapy following successful induction of remission following rescue therapy is relatively limited. Data to guide the optimal maintenance strategy following successful induction of remission with sequential therapy or third-line strategies are also lacking.
Data from a retrospective multicenter French study found lower rates of relapse after a first episode of ASUC in those treated with anti-TNF containing maintenance regimens compared to those containing 5-aminosalicylates or conventional immunosuppressants [74].
In biologic-naïve patients, 5-aminosalicylates and/or azathioprine with or without combination infliximab can be used. The use of maintenance azathioprine compared to azathioprine in combination with infliximab is currently being investigated in the ACTIVE trial (NCT02425852) among IV steroid responders and PREDICT UC (NCT02770040) among IV steroid-refractory patients.
In previous failure of infliximab, drugs that are yet to be evaluated in clinical trials include vedolizumab, ustekinumab, and JAK-inhibitors.
Vedolizumab, a selective anti-adhesion monoclonal antibody targeting α4β7 integrin has been demonstrated to be effective in moderate to severe UC [75]. Vedolizumab prevents α4β7 integrin interaction with MAdCAM-1 expressed on gastrointestinal epithelial cells, thereby inhibiting T-cell migration into intestinal tissue. Its slow onset of action limits its use in ASUC; however, it can be used in combination with a rapid-acting agent such as IV steroids or cyclosporin rescue as a bridge to vedolizumab maintenance [76].
The safety and effectiveness of vedolizumab has been evaluated in a recent systematic review by Gisbert et al. of 8 studies [34,76-83]. The majority of studies were retrospective, included patients who had failed anti-TNFs and most used cyclosporin as bridge to vedolizumab. The colectomy-free rate in patients treated with vedolizumab for ASUC was 69% (weighted mean 95% CI, 61%-76%) and the rate of serious adverse events (or adverse events leading to discontinuation) was 1.8% with no mortality due to cyclosporin or vedolizumab [34]. Since then, another successful case of cyclosporin rescue as a bridge to vedolizumab has been reported by Ashat et al. [84]. Hence, calcineurin inhibition as a bridge to vedolizumab maintenance therapy appears to be a safety and effective strategy in patients with ASUC.
Ustekinumab, a monoclonal antibody targeting the p40 subunit of IL-12 and IL-23, has also been shown to be effective in patients with moderate to severe UC. Use of cyclosporin/tacrolimus as a bridge to ustekinumab in ASUC has been evaluated in 3 small retrospective studies comprising a total of 13 patients who had previously failed anti-TNF and/or vedolizumab [34,85-87]. Colectomy was avoided in all patients with no severe adverse events or mortality observed with either agent [34].
In a recent prospective study of 11 patients with steroid-refractory ASUC (10 of whom were biologic experienced, and 8 of whom had previously failed ≥ 3 biologic therapies), ustekinumab was commenced after a mean of 3.2 weeks after initiation of cyclosporin rescue, and combination therapy continued for a mean of 11.5 weeks. Six patients (54%) were clinical responders at week 16, with 5 patients (45%) in endoscopic remission at the same time point. At long-term follow-up at 52 weeks, 5 patients (45%) were in histological remission [88].
Hence, although the data are limited calcineurin inhibition as bridge to ustekinumab maintenance therapy may be a safe and effective strategy in ASUC, even in the setting of prior biologic treatment experience.
The JAK-inhibitors tofacitinib, upadacitinib and filigotinib are effective in MSUC [89-91]. Potential benefits of these agents include their oral administration, relatively rapid onset of action, ease of transition from induction to maintenance therapy and lack of immunogenicity. However, data regarding the safety and efficacy of these agents to maintain remission following successful induction of remission in ASUC are awaited.
WHEN TO CONSIDER COLECTOMY
The evolving nature of therapeutic approaches and availability of new drugs for ASUC has increased the complexity behind decision making as to when it is appropriate to proceed to colectomy. The time to clinical response of individual drugs varies from patient to patient, hence decision making is a day-by-day proposition. In the absence of validated predictive indices of therapeutic response to rescue therapies, one should proceed to colectomy if there is a negative trend in: clinical indices (comprised of vital signs, rectal bleeding and abdominal tenderness), biomarkers (rising CRP), colonic dilatation on abdominal imaging or endoscopic deterioration. Monitoring of such parameters is all the more important in the setting of sequential therapy. Decision making regarding when to proceed to colectomy therefore involves timely risk assessment, assessment of treatment response and multidisciplinary team management.
DISCUSSION
The treatment landscape of ASUC is rapidly evolving with new rescue therapy options, although most of these are still under evaluation. Whilst the traditional therapies of infliximab and cyclosporin remain the mainstays of treating steroid-refractory disease, these therapies are not always effective. Hence, attention has shifted towards investigating mechanisms of drug failure, predicting non-response to therapy and devising strategies to overcome non-response.
Non-response or incomplete response to infliximab may be driven by increased infliximab clearance, tissue mediated drug deposition or alternate non-TNF mediated pathways [35]. While incomplete response may be overcome by dose optimization via accelerated or intensified dosing, the optimal infliximab dosing strategy is yet to be defined and is the subject of ongoing trials (NCT03937609 and NCT02770040). Non-response to infliximab in ASUC that cannot be overcome by dose optimization suggests the need for sequential therapy to address alternate non-TNF mediated pathways. While cyclosporin has represented a feasible alternative in such patients, preliminary data suggest that JAK inhibitors may be safe and effective as sequential therapy and therefore require further investigation in relation to their safety, efficacy, role and positioning as rescue therapy agents.
Despite its more challenging route of administration cyclosporin is enjoying a renaissance in some centers familiar with its use. Not only is cyclosporin being used among those who are thiopurine and infliximab naïve but it is also finding a role as a bridging therapy induction agent to allow slower acting biologic therapies such as vedolizumab and ustekinumab to take effect as maintenance agents.
A unique advantage of JAK inhibitors is their capacity to act as both a rescue therapy option as sequential therapy as well as a maintenance agent following successful induction; however, the optimal dosing regimen for both induction and maintenance also requires further investigation.
Whilst advanced therapies have traditionally been used in the setting of steroid non-response (failure) in ASUC, the treatment paradigm may shift in the future with the potential use of JAK inhibition either as an alternative or adjunct to IV steroids. In the recent TACOS study, patients with ASUC were randomized to a 7-day course of tofacitinib 10 mg TDS or placebo TDS while continuing IV hydrocortisone, and treatment response was assessed at day 7 [92]. Patients who responded to tofacitinib received tofacitinib 10 mg BD maintenance therapy whereas steroid monotherapy responders received oral 5-aminosalicylates and thiopurine therapy. Patients who received tofacitinib were more likely to be treatment responders compared to those who received placebo (83.01% vs. 58.82%; OR, 3.42; 95% CI, 1.37-8.48; P= 0.007). Similarly, patients in the tofacitinib group were less likely to require rescue therapy at 7 days (OR, 0.27; 95% CI, 0.09-0.78; P= 0.01) and at 90 days compared to those in the placebo group (cumulative probability 0.13 vs. 0.38 respectively, P= 0.003) [92]. Although most adverse events were mild, there was 1 case of dural venous thrombosis in the tofacitinib arm [92]. Whilst the use of tofacitinib as an adjunct to steroids seems promising, such an approach may risk over-treating patients who will respond to conventional therapy. Similar to calcineurin-inhibitor treatment, JAK inhibitors may be used as induction therapy to bridge to selective therapies with more favorable safety profiles.
Although infliximab and cyclosporin have traditionally been used as first-line rescue therapies, 2 small recent case series have examined the use of tofacitinib as first-line rescue therapy in steroid-refractory patients with ASUC, in predominantly biologic-naïve cohorts [93,94]. Short-term clinical response rates in both series were promising and in the order of 75% to 88% (Table 2). However, the serious adverse events included a case of herpes zoster and 2 deaths, including 1 occurring in a patient who developed sepsis after colectomy, and 1 who died of bacterial pneumonia 1 month after commencement of tofacitinib [93,94]. These preliminary data suggest that although effective, first-line tofacitinib rescue may be associated with significant risks and therefore warrants further evaluation of safety and efficacy within controlled clinical trials.
CONCLUSIONS AND FUTURE DIRECTIONS
In the setting of a broadening armamentarium of traditional versus novel rescue therapies and dosing regimens it is difficult to establish the optimal timing, dosing, and duration of each successive rescue therapy agent. Novel strategies and predictive indices of rescue therapy response are currently under development in ASUC to help with decision-making regarding each of the rescue therapies and to determine the specific parameters that define therapeutic success or failure. Whilst randomized controlled trials are ideally required to discern the positioning of advanced therapies in ASUC, such trials are often not practical to conduct in the setting of failure of first-line rescue therapy. Hence, data to guide management following failure of first-line rescue are more likely to come from both real-world and modeling studies. Irrespective of the advances in medical therapy, knowing when to proceed to colectomy requires timely risk assessment, assessment of treatment response and multidisciplinary management. Colectomy constitutes an appropriate intervention for treatment refractory disease and should therefore not be considered a failure of contemporary ASUC management.