INTRODUCTION
Ulcerative colitis (UC) is a chronic, idiopathic inflammatory bowel disease (IBD) characterized by relapsing abdominal pain and bloody diarrhea with or without mucus [1]. The incidence and prevalence of UC have been reported as high in Northern Europe and North America and low in Asian countries [2-5]. However, researchers recently observed an increased number of UC patients in Asian countries including Korea, Japan, China, and Taiwan [6-8]. The incidence of UC in Asia has been rising in relation to rapid urbanization and a westernized lifestyle [9,10]. A population-based study performed in Korea showed that the incidence and prevalence of UC have been gradually increasing [10,11]. Furthermore, the genetic and clinical characteristics of IBD patients from Asia and Western countries are slightly different [12,13].
Adalimumab (ADA) is a fully human immunoglobulin G1 monoclonal antibody directed against tumor necrosis factor-Ī± (TNF-Ī±) that inhibits the activity of the cytokine by blocking the interaction of TNF-Ī± with its p55 and p75 cell surface receptors [14]. In Korea, ADA has been administered to patients with UC since 2013, and a nationwide population-based study showed that 27.6% were treated using ADA among patients who received anti-TNF-Ī± therapy [10].
Till date, little information regarding the clinical outcomes of the use of ADA in the Korean population is available. Most published studies of clinical outcomes in IBD have been conducted on Western patients. Investigating the clinical outcomes of biologic agents in Korean IBD patients will enable a better understanding and optimal management of this condition. Therefore, we conducted a prospective, observational, multicenter study to evaluate the real-world efficacy and safety of ADA and predictors of response in Korean patients with UC.
METHODS
1. Patients
This prospective, observational, multicenter study was conducted at 17 academic hospitals in Korea from June 2015 to September 2018. The study protocol was approved by the institutional review board at each center (IRB No. C2015020) and registered at clinicaltrials.gov (study identifier: NCT02499263). All patients provided written informed consent. All work was carried out in compliance with the Ethical Principles for Medical Research Involving Human Subjects outlined in the Helsinki Declaration in 1975 (revised in 2000). All authors had access to the study data and reviewed and approved the final manuscript.
Eligible patients were aged > 18 years and had moderately to severely active UC defined as a Mayo score [15] between 6 to 12, with an endoscopic subscore of at least 2, despite concurrent therapy with 5-aminosalicylic acid, corticosteroids, and azathioprine/6-mercaptopurine. Previous use of anti-TNF-Ī± agents other than ADA was permitted if the patient had discontinued its use owing to primary nonresponse, loss of response, or intolerance to the agent. Exclusion criteria were contraindications for using ADA including malignancy; severe infection such as active tuberculosis, invasive fungal infection, and opportunistic infection; being enrolled in other clinical trials; and pregnancy or breastfeeding. Patients were excluded if they chose to withdraw from the study or if the investigator discontinued ADA because of ethical or practical conflicts. Baseline assessment performed before administration of ADA, and details can be found in supplementary section.
2. Study Design
Patients received subcutaneous injections of ADA: 160 mg at week 0, 80 mg at week 2, and 40 mg every alternate week from week 4. Patients were evaluated at weeks 0 (baseline), 8, 16, 24, 32, 40, 48, and 56 in accordance with clinical practice. The window period was permitted as Ā± 1 week for every visit. All participants underwent safety evaluations ā¤ 30 days after the last administration of ADA.
Analysis of Mayo scores, including endoscopic subscore, and fecal calprotectin (FC) levels and laboratory tests, were performed at weeks 8 and 56. ADA trough level was evaluated at week 8 and at loss of response, even if ADA dose escalated to weekly injection. Patients with inadequate response to ADA (40 mg every 2 weeks) were permitted to escalate the dosage to 40 mg every week. Patients with inadequate response to dose escalation discontinued the drug based on their physicianās judgement. Inadequate response was defined in supplementary section.
3. Outcomes
The primary outcomes were clinical response rates at weeks 8 and 56. Clinical response was defined as a decrease in Mayo score from baseline by ā„ 3 points and ā„ 30% with an accompanying decrease in rectal bleeding subscore of ā„ 1 point or an absolute rectal bleeding subscore of 0 or 1. Secondary outcomes were proportion of patients with clinical remission, steroid-free remission, and mucosal healing at weeks 8 and 56. Clinical remission was defined as a Mayo score ā¤ 2 with no individual subscore exceeding 1 point. Steroid-free remission was defined as a clinical remission status with no use of systemic corticosteroids for 12 weeks before the date of investigation. Mucosal healing was defined as an endoscopy subscore of 0 or 1. Endoscopic remission was defined as an endoscopic subscore of 0. Predictors of response at weeks 8 and 56 were evaluated based on clinical characteristics at baseline and week 8. Safety evaluation was performed according to the recent version of the Medical Dictionary for Regulatory Activities version 20.0. Physical examination, investigation of vital signs, and laboratory tests were performed from baseline to week 56 and after 30 days from the last administration.
4. Statistical Methods
Analyses were performed with the intent-to-treat set. Missing or incomplete data were handled using the nonresponder imputation method, i.e., patients with missing or incomplete data were assumed to have not achieved the endpoint. Continuous variables are described with the number of subjects, arithmetic mean, and standard deviation. For categorical variables, the frequency and proportion are presented. For all the statistical tests, two-sided tests were conducted at the 0.05 significance level using the independent or paired t-test and the chi-square test. To identify factors associated with clinical response at weeks 8 and 56, variables that were significant in univariate analysis were subsequently tested in multivariate logistic regression analysis and expressed as odds ratios (ORs) with 95% confidence intervals (CIs). The Kaplan-Meier method was used to evaluate the drug persistence rate. All statistical analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA).
RESULTS
1. Primary Endpoint
A total of 146 patients from 17 academic hospitals in Korea were enrolled and included in the analysis. Table 1 summarizes the baseline clinical characteristics of the participants.
Clinical response was achieved in 52.1% (76/146) of the patients at week 8 and 37.7% (55/146) of the patients at week 56 (Fig. 1A). Clinical response rate at week 56 in week 8 responders was 54.0% (41/76). Clinical response rate was not significantly different between patients who received anti-TNF-Ī± and those who did not (Fig. 1B and C). The combination therapy with azathioprine/6-mercaptopurine in baseline was not associated with clinical response rate at both weeks 8 and 56 (Fig. 1D).
2. Secondary Endpoints
At week 8, 24.0% (35/146) of patients were in clinical remission, and 22.0% (32/146) of patients achieved clinical remission at week 56. Steroid-free clinical remission was achieved in 12.3% (18/146) of patients at week 8 and 21.2% (31/146) of patients at week 56. Mucosal healing was achieved in 39.0% (57/146) of patients at week 8 and 30.1% (44/146) at week 56 (Fig. 1A). Rates of clinical remission and mucosal healing were not significantly different between patients who received anti-TNF-Ī± and those who did not (Fig. 1B and C). Twenty-five patients (17.1%) experienced dose escalation, and 40% and 20% of these achieved clinical response and remission at week 56, respectively.
3. Comparison of Clinical Characteristics between Clinical Responders and Nonresponders
A comparison of clinical characteristics between clinical responders and nonresponders can be found in Tables 2 and 3. Higher body mass index (BMI) (P=0.034) and serum albumin level (P=0.019), and less severe endoscopic findings (P=0.002) at baseline were associated with clinical response at week 8. Higher baseline BMI (P=0.017), and clinical response (P<0.001) and mucosal healing (P=0.008) at week 8 were associated with clinical response at week 56. Mayo score (P=0.026) and serum C-reactive protein (CRP) level (P=0.035) at week 8 were significantly lower in clinical responders than in nonresponders at week 56. In the multivariate analysis, baseline non-severe endoscopic finding (OR, 2.951; 95% CI, 1.365-6.382; P=0.006) and clinical response (OR, 10.456; 95% CI, 1.903-57.458; P=0.007) at week 8 were independent predictive factors for clinical responses at week 8 and week 56, respectively (Table 4).
4. Exploratory Outcomes
Treatment persistence rate and causes of discontinuation can be found in Supplementary Fig. 1 and Supplementary Table 1. Clinical response rates according to the partial Mayo score can be found in Supplementary Fig. 2.
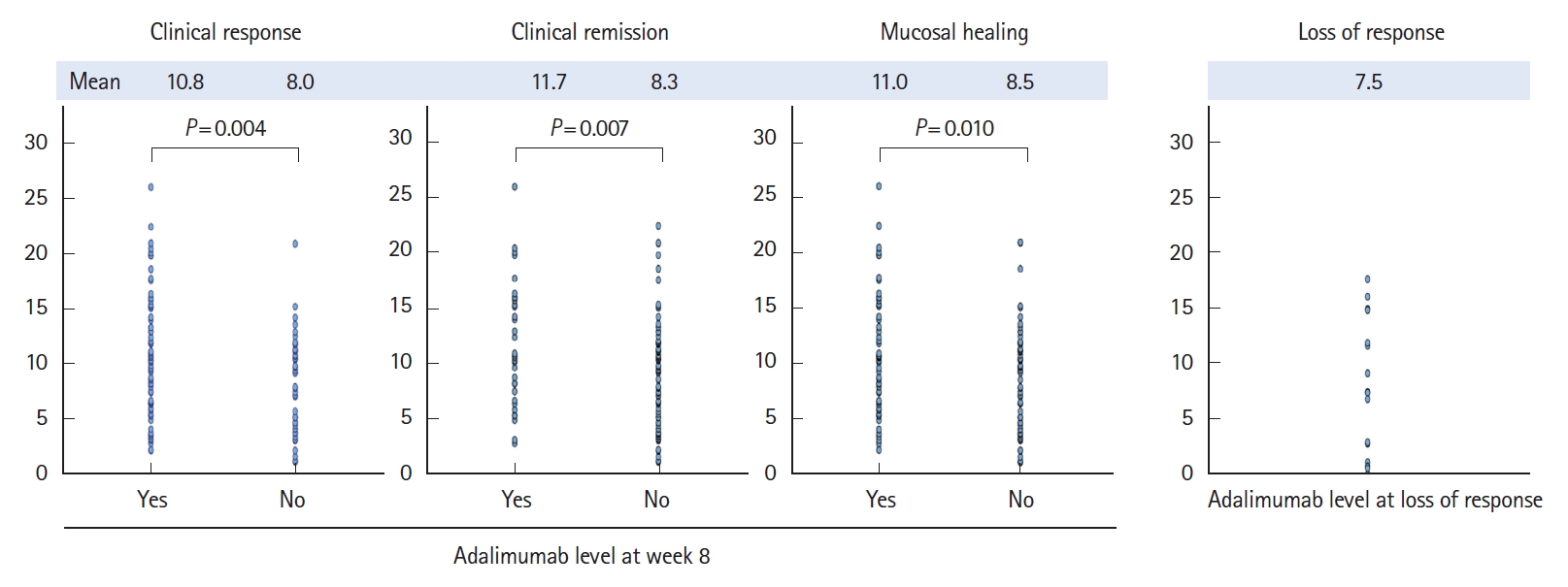
Mean serum ADA concentration (trough level, Ī¼g/mL) was significantly higher in patients who achieved clinical response (10.8 vs. 8.0, P=0.004), remission (11.7 vs. 8.3, P=0.007), and mucosal healing (11.0 vs. 8.5, P=0.010) than in those with no clinical response at week 8. Mean serum ADA level was 7.5 Ā± 6.4 Ī¼g/mL (range, 0.1-17.7 Ī¼g/mL) in patients who stopped ADA administration because of inadequate response (Fig. 2). FC and CRP levels associated with the clinical and endoscopic outcomes can be found in Fig. 3.
A total of 246 FC levels were collected at the 3 points, and the correlation with endoscopic findings was investigated by integrating them (Fig. 4). The FC level to predict mucosal healing was 274.7 mg/kg, with a sensitivity of 72.2% and specificity of 71.3% on the receiver operating curve (area under the curve, 0.771). The predictive level for endoscopic remission (Mayo subscore 0) was 87.9 mg/kg, with a sensitivity of 73.6% and specificity of 73.5% on the receiver operating curve (area under the curve, 0.774).
5. Safety
During the study period, 6.2% (9/146) of patients experienced adverse drug reactions. Serious adverse drug reactions that induced hospital admission were identified in 2.8% (4/146) of patients as follows: pneumonia, pulmonary tuberculosis, renal failure, and abdominal pain (Supplementary Table 2).
DISCUSSION
In this prospective multicenter study, we evaluated the real-world clinical effectiveness of ADA treatment and factors associated with the clinical response in Korean patients with moderately to severely active UC. Our study showed similar or slightly higher rates of clinical response and remission than 2 previous pivotal studies conducted in Western countries: ULTRA-1 and ULTRA-2 (response rates, 50.4%-54.6%; remission rates, 16.5%-18.5% at week 8 and 30.2%-17.3% at week 52) [14,16]. Several studies investigating the real-world efficacy of ADA have been reported worldwide. Although it is difficult to directly compare these results, because each study defined clinical response and remission differently, they show similar trends in outcomes [17-19]. A Japanese real-world study that applied the same definition for clinical response and remission as this study, reported similar outcomes [17]. The mucosal healing rate in our study tended to be lower than that reported in previous Western studies [18,19], but similar to that reported in a Japanese study [17]. Collectively, ADA was similarly effective for induction and maintenance treatments in Korean patients with active UC who were unresponsive to corticosteroids and/or azathioprine/6-mercaptopurine.
Previous experience with anti-TNF-Ī± therapy was not found to impact the short- or long-term outcomes in our study. Prior anti-TNF-Ī± therapy has been reported to have controversial effects on clinical outcomes of ADA in patients with UC. The ULTRA-2 and ULTRA-3 studies reported better outcomes in patients not treated with anti-TNF-Ī± [14,20]. A retrospective multicenter study in Spain investigated the influence of previous anti-TNF-Ī± use on the outcomes of ADA maintenance treatment in patients with UC; patients not previously treated with anti-TNF-Ī± had a numerically higher rate of clinical response at week 56 without statistical significance [21]. They had significantly lower probabilities of avoiding colectomy and dose escalation. However, in a previous Hungarian prospective study, response to ADA and need for dose escalation were not associated with previous infliximab (IFX) therapy [19]. A retrospective study performed in Ireland showed a trend towards better outcomes in patients previously received anti-TNF-Ī± compared with those who were not [22]. It is difficult to explain this inconsistency. Relatively small portion of patients with antiTNF-Ī± (n=36, 24.7%), and higher rate of dose escalation in patient with anti-TNF exposure (41.9%) compared with anti-TNF naĆÆve patients (9.0%) (data not shown) in our study may affect the results. Although a note of caution is due, ADA can be suggested as a beneficial option for Korean patients with moderately to severely active UC treated previously with anti-TNF-Ī± therapy. In addition, the combination therapy with azathioprine/6-mercaptopurine did not affect clinical response rate. This finding is consistent with that of previous studies showing no efficacy-related benefits following immunomodulator/ADA combination therapy [20,23,24].
In this study, baseline BMI, endoscopic findings, and serum albumin level were associated with clinical response at week 8. At week 56, baseline BMI and clinical response, mucosal healing, CRP level, and Mayo score at week 8 were associated with clinical response. In the multivariate analysis, baseline non-severe endoscopic finding and clinical response at week 8 were independent factors for predicting response at weeks 8 and 52, respectively. Although it was a significant factor only in the univariate analysis, BMI was associated with both short- and long-term response. Previous studies have shown that obese patients tended to have higher risk of nonresponse to biologic agents because of their direct effect on inflammation and modification of pharmacokinetics [14,25,26]. However, average BMI of both responder and nonresponder groups were within the normal range in our study. Relatively higher BMI within the normal range might reflect less severe disease status. CRP level has been suggested as a predictor of poor outcome in UC patients [27] and considered a biomarker of response to IFX induction therapy [28,29]. Endoscopic finding is also one of the major factors determining the severity and prognosis of UC. In this study, the baseline CRP levels were lower in responders than in nonresponders, though without statistical significance. The less severe endoscopic activity was associated with better response to induction therapy of ADA. The findings from this study suggest that ADA therapy may be more effective in moderately active UC than in severely active UC.
Parameters associated with early response such as mucosal healing, clinical response, and CRP level were associated with long-term response. Mucosal healing has been reported to be associated with long-term clinical outcomes [18,30] and suggested as a predictive factor of long-term outcome in Korean UC patients treated with IFX [31]. Early clinical response has also been demonstrated as a predictive factor of better long-term clinical outcomes in several real-world studies [17,32,33]. In Korean patients with moderately to severely active UC, early response is also a positive predictor for long-term clinical response.
During the study period, 25 patients (17.1%) required dose escalation, and 40% and 20% of these regained clinical response and remission, respectively, at week 56. Compared to previous Western studies, the proportion of patients who experienced dose escalation in our study was relatively small; however, the clinical outcomes are similar to those of these studies [21,34,35].
Consistent with previous studies on mucosal healing-associated FC levels [36-38], in this study, FC levels were well correlated with not only patientsā clinical outcomes, but also endoscopic activities. The predictive level was 274.8 mg/kg for mucosal healing and 98 mg/kg for endoscopic remission. These novel findings can be used to predict endoscopic activities in UC patients.
Serum ADA concentrations (trough level) at week 8 were associated significantly with clinical outcomes of induction therapy. The mean ADA concentrations in patients without clinical response, remission, and mucosal healing were relatively higher compared with those in previous studies [39-41]. It can be assumed that different mechanisms other than signaling pathway via TNF may be involved in the development of UC in these patients. In addition, most previous studies included both patients with UC and Crohnās disease, and few studies have been conducted to investigate ADA concentration in patients with UC only. A Belgian study including IFX responders and nonresponders showed similar ADA concentrations as those in this study with respect to short-term mucosal healing [42]. The researchers reported that the average ADA concentration of patients with mucosal healing at week 4 was 10.6 Ī¼g/mL, which was significantly higher than the concentration in those without mucosal healing (7.4 Ī¼g/mL, P=0.014). More real-world data may be needed to establish optimal level for treatment target, but our finding suggests that the higher the drug concentration at week 8 after ADA induction therapy, the better was the expected clinical effect.
No new safety signals were observed in the present study, and the incidence rate was similar to that described in other studies [18,43]. Any different tendency in safety from the approved label of ADA was not observed. Patients with severe adverse drug reactions including abdominal pain and pulmonary tuberculosis were treated properly, and no deaths were reported.
This was an observational study in routine clinical practice, having certain inherent limitations such as the lack of randomization, leading to potential bias. Moreover, the proportion of subjects who completed the evaluation without any major protocol deviation among the intent-to-treat set was relatively small. Therefore, with a small sample size, these data must be interpreted with caution. Furthermore, anti-ADA antibodies were not evaluated in this study, although it is used in clinical practice in Western countries. However, this study was the first multicenter prospective study to evaluate the efficacy and safety of ADA in Korean UC patients in the real-life clinical setting and explore clinical predictors of response to ADA, including FC and ADA drug levels.
In conclusion, this study showed that ADA is effective and safe for Korean patients with moderately to severely active UC regardless of prior anti-TNF-Ī± therapy. ADA drug level is associated with the efficacy of induction therapy. A good response to induction therapy suggests positive long-term outcomes in Korean patients with moderately to severely active UC.