INTRODUCTION
Primary sclerosing cholangitis (PSC), a chronic progressive inflammatory disease of the intrahepatic and/or extrahepatic bile ducts, represents the main hepatobiliary extraintestinal manifestation of inflammatory bowel disease (IBD) [1,2]. The prevalence of PSC in IBD (PSC-IBD) varies between 3% to 8% for patients with ulcerative colitis (UC) and 2% to 3% for patients with CrohnŌĆÖs disease (CD), while PSC is associated with IBD in 50% to 90% patients [3,4]. Though the exact pathogenesis of both IBD and PSC are not known, the 2 are believed to share a common pathophysiology, influenced by immune-mediated processes (gut lymphocyte homing), immunogenic susceptibility, increased intestinal permeability, dysbiotic gut microbiota, genetic predisposition, disorders of biliary epithelial cells and altered bile acid metabolism [5-9]. The PSC-IBD has been described as a unique entity, different from IBD, characterized by an increased incidence of pancolitis, backwash ileitis, and rectal sparing; though the colitis tends to be clinically and often endoscopically quiescent [10-13]. An increased risk of colorectal cancer (CRC) in patients with PSC and IBD drives the differences in approach to management of PSC with IBD as compared to IBD alone, the former including lifelong annual surveillance colonoscopy [14-17].
Though the association between PSC and IBD is well recognized, there remains uncertainty on the magnitude of the problem. A recent systematic review and meta-analysis estimated the global prevalence of PSC in patients with IBD at 2.16%, with appreciable regional variations [18]. Limited data exist on the prevalence and disease phenotype of PSC with IBD from India [19,20]. This multicenter study aimed to investigate the prevalence of PSC with IBD, describe the disease phenotype (clinical features, disease characteristics, and disease-related complications) and evaluate regional variations in the spectrum of PSC in patients with IBD in India.
METHODS
1. Study Design
This study is a retrospective analysis of prospectively maintained IBD databases at 5 tertiary care centers across India: Dayanand Medical College and Hospital, Ludhiana (north India); All India Institute of Medical Sciences, New Delhi (north India); Postgraduate Institute of Medical Education and Research, Chandigarh (north India); P.D. Hinduja National Hospital and Medical Research Centre, Mumbai (west India); and Asian Institute of Gastroenterology, Hyderabad (south India). The respective databases were reviewed for a period between January 1991 and December 2020. The study was approved by the Ethics Committee of Dayanand Medical College and Hospital (IRB No. DMCH/R&D/2020/23). This study is a retrospective study and so informed consent was waived. A proportion of the patients reported in the current study were also included in a previous single-center study describing the prevalence and spectrum of extraintestinal manifestations in patients with IBD [19].
2. Study Population
Patients with established diagnosis of IBD (based on the European CrohnŌĆÖs and Colitis Organisation and European Society of Gastrointestinal and Abdominal Radiology Guidelines) who were found to have concomitant PSC (diagnosed on the basis of biochemical cholestasis [elevated alkaline phosphatase] and cholangiographic evidence of strictures/ectasias of intrahepatic and/or extrahepatic bile ducts) were included for analysis [21,22].
The details on demographic profile (including age at diagnosis of PSC-IBD and sex), clinical history (disease diagnosis, clinical presentation, disease extent, severity, and behavior), complications including cirrhosis, CRC and cholangiocarcinoma (CCA) and medical/surgical treatment were extracted from the databases. Montreal classification was used to assess the disease phenotype in adults with IBD. Disease severity was defined by the Mayo Clinic score in patients with UC and Harvey Bradshaw Index in patients with CD.
Patients with missing/incomplete data, follow-up < 6 months and a secondary cause for sclerosing cholangitis (such as infectious or ischemic cholangiopathy, IgG4 associated cholangitis, portal cavernoma cholangiopathy, drug-induced liver injury, choledocholithiasis, and surgical trauma to biliary tract) were excluded.
3. Statistical Analysis
Quantitative data were presented as mean ┬▒ standard deviation or median and interquartile range (IQR). Categorical data were summarized as the percentage of the group total. Categorical data were compared using either the chi-square test (for parametric data) or the Kruskal-Wallis one-way analysis of variance test (for non-parametric data). Fischer exact test was performed when the anticipated frequency was less than 5. A probability value (P-value) less than 0.05 was considered statistically significant. All statistical calculations were done using SPSS version 21 (IBM Corp., Armonk, NY, USA) statistical program for Microsoft Windows.
RESULTS
1. Prevalence of PSC in Patients with IBD
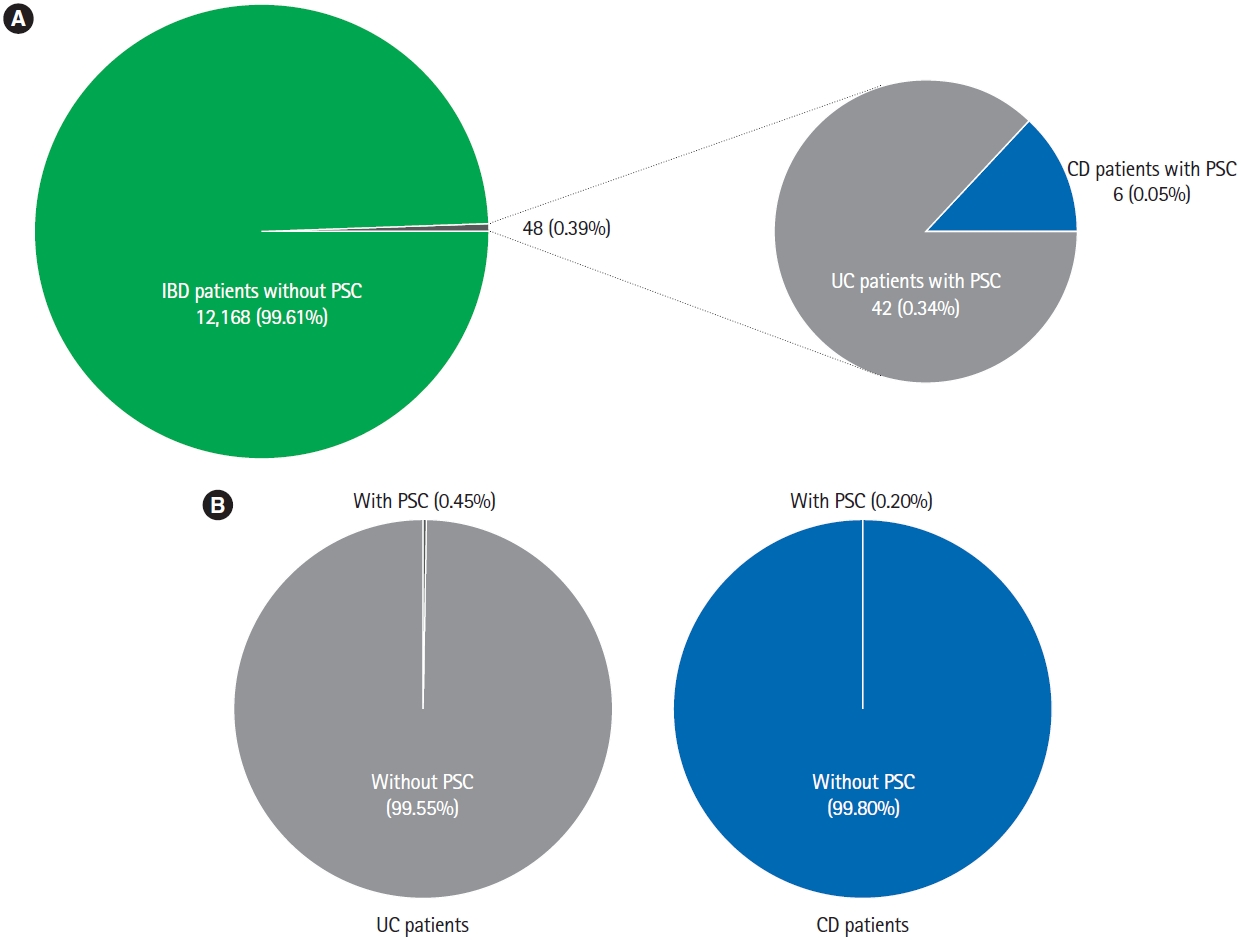
Records of 12,216 patients with IBD (9,231 UC, 2,939 CD, and 46 IBD unclassified) were analyzed. Forty-eight patients were identified to have PSC, resulting in a prevalence of 0.39%. Of the 48 patients diagnosed with PSC, 42 (87.50%) had UC while 6 (12.50%) had CD. The cumulative prevalence of PSC was 0.45% in patients with UC and 0.20% in patients with CD (Fig. 1). The mean Mayo Clinic score and Harvey Bradshaw Index were 5.26 ┬▒ 2.41 and 5.17 ┬▒ 1.33 in patients with UC-PSC and CD-PSC, respectively.
2. Characteristics of the IBD Patients Diagnosed with PSC
Majority of the patients (n = 27, 56.25%) were males. In nearly 70% of the patients, the diagnosis of IBD preceded the diagnosis of PSC with a mean duration of 43.25 ┬▒ 74.66 months between the diagnoses of the 2 entities. In only 4 patients (8.33%), PSC was diagnosed before the diagnosis of IBD was established. Approximately two-thirds (69.05%) of the patients with UC-PSC had pancolitis, while isolated colonic involvement (50%) followed by ileo-colonic disease (33.33%) was the most common disease location in patients with CD-PSC. The frequency of stricturing and/or penetrating disease was low (16.66%) in patients with CD-PSC. The clinical characteristics of the patients with PSC and IBD are summarized in Table 1.
3. Clinical Presentation and Complications of PSC in Patients with IBD
A majority of the patients (n = 32, 68.75%) were symptomatic for liver disease at the time of diagnosis of PSC-IBD. The common presenting symptoms were fatigue (n = 31, 64.58%), abdominal pain (n = 14, 29.16%), pruritus (n = 12, 25%), and jaundice (n = 7, 14.58%). One patient had cirrhosis at the time of diagnosis of PSC (Table 2). The median alkaline phosphatase at the time of diagnosis was 417.0 IU/L (IQR, 293.5-637.0 IU/L). All the patients had evidence of cholangiographic changes of beading/stricturing and/or ectasias.
The patients were followed up for a median of 66 months (IQR, 27-129 months). During the follow-up period, 7 more patients developed cirrhosis. Five patients (10.41%), all UC, developed malignancies (3 CRC [6.25%] and 2 CCA [4.16%]) (Fig. 2). Three patients died during follow-up (2 decompensated liver disease and 1 CCA) (Table 2).
All the patients were on concomitant therapy with ursodeoxycholic acid for PSC. Eight patients with dominant biliary strictures required endoscopic balloon dilatation. Two patients needed liver transplant for decompensated liver disease, while another 2 underwent colectomy with adjuvant chemotherapy for CRC. Three patients (2 CCA and 1 CRC) received palliative chemotherapy for associated malignancy. None of the patients mandated surgical therapy for IBD (Table 2).
DISCUSSION
This multicenter study evaluated the relationship and characteristics of IBD and PSC in a large cohort of IBD patients from India. The prevalence of PSC in patients with IBD was 0.39%. The prevalence of PSC in UC and CD separately was 0.45% and 0.20%. The prevalence rate in the current study is lower than the reported prevalence in previous studies from Westernized countries [18,23,24]. However the PSC prevalence rate in IBD is similar to previously reported rates of 0.3% in India and 0.48% in the Inflammatory Bowel Disease-Emerging NationsŌĆÖ Consortium [19,20]. PSC (with or without concomitant IBD) exhibits wide variations in its geo-epidemiology, with lower prevalence rates reported from Asia as compared to North America and Europe. The prevalence rates of PSC-IBD in the current study are amongst the lowest, even in Asia [18]. This could be attributed to heterogeneity in genetic, ethnic, environmental, and other risk factors that lead to development of PSC, suggesting that though the disease phenotypes maybe similar, demographic differences exist in IBD among Asian and Western countries [25].
Majority of the patients with PSC-IBD (both UC and CD) concurrence were males (56.25%) and had their IBD diagnosed before PSC (70%). The ratio of UC-PSC and CD-PSC concurrence in the current study was 7:1, indicating higher prevalence of PSC in patients with UC as compared to CD. Consistent with the previous reports, pancolitis and colonic disease location were the commonest disease extent and location in patients with UC and CD respectively, suggesting colonic involvement as the hallmark of the PSC-IBD phenotype. However, in contrast to the earlier studies, where none of the patients with proctosigmoiditis had PSC, 30% of UC-PSC patients in the current study had proctosigmoiditis (disease extent E2) [26-28]. Whether this represents a distinct phenotype of PSC-IBD that behaves differently form the pancolitis associated PSC-IBD is not known and needs to be evaluated. Only 6.25% of patients with PSC-IBD were current or former smokers. This is congruous with decreased risk of PSC among smokers described earlier [29].
Most of the patients with PSC-IBD were symptomatic at diagnosis. This is in contrast to the earlier descriptions of PSC being asymptomatic and detected on screening for liver disease in patients with IBD [30]. A higher proportion of patients being symptomatic in the current study could either imply late diagnosis of PSC due to challenges in adhering to PSC screening protocols [31] or a different spectrum of PSC-IBD in India. Although statistically insignificant, a greater proportion of patients with CD-PSC developed cirrhosis. On the contrary, malignancies (either CRC or CCA) developed more frequently in patients with UC-PSC. The rates of liver transplantation and death were lower in patients with CD-PSC. Though evaluating the effect of IBD type on the clinical presentation and complications of PSC-IBD was not the objective of the current study, our findings suggest a natural history of CD-PSC distinct from the UC-PSC. Similar findings have been reported previously, where patients with CD-PSC progressed less commonly to cancer, liver transplantation, or death [32,33].
Approximately 10% of the patients with PSC-IBD progressed to develop malignancies. The prevalence of CRC and CCA in PSC-IBD was 6.25% and 4.17%, respectively. CCA has been reported to develop in up to 5%-20% of patients with PSC [34,35]. The prevalence of CRC in patients with IBD varies between 2%-3% in India and increases substantially in the second and third decade after the onset of IBD even though the incidence of sporadic CRC is low [36-38]. This paradox suggests that inflammation-driven CRC has similar incidence rates in the East as well as the West. Though the prevalence of CRC in PSC-IBD is twice the prevalence in UC without PSC, the rates are much lower than the 20% to 30% prevalence rates described previously [39,40]. The lower rates of CRC can be attributed to distinct genetic and gut microbial composition of Indians as compared to the Caucasians, apart from variations in the Farnesoid X receptor and bile acid metabolic pathways, which play an integral role in the development of malignancies in patients with PSC-IBD [41-43]. The lower incidence of CRC in the present cohort could also possibly be related to a shorter follow-up period and low annual CRC screening rates. More prospective longitudinal studies are needed to better determine the natural history and formulate cost-effective population specific policies for surveillance of cancers in PSC-IBD patients.
This study is the first nationwide study determining the prevalence of PSC in patients with IBD from India. The strengths of our study include large sample size and strict criteria of a combination of biochemical cholestasis and positive cholangiography for diagnosis of PSC. However, retrospective nature of the study may have resulted in an underestimation of the true prevalence of PSC-IBD as patients with missing data were excluded. Patients with PSC who do not have clinical symptoms of IBD may have endoscopic and/or histological features consistent with IBD. As patients with PSC who did not have intestinal symptoms were not evaluated in the current study, underreporting of the prevalence of PSC-IBD is possible, though the proportion of such patients is expected to be small. Data on liver biopsy was not available and therefore patients with small duct PSC or patients with normal biochemistry could have been missed. Additionally, the details on proportion of patients with backwash ileitis and rectal sparing, reportedly more prevalent in patients with PSC-IBD, were not available.
In conclusion, this multicenter nationwide study demonstrates low prevalence rates (0.39%) of PSC in patients with IBD in India. Males, patients with UC and patients with pancolitis (UC) or colonic CD were more likely to receive a diagnosis of concomitant PSC and IBD. Majority of the patients were symptomatic of PSC at the time of diagnosis. The prevalence of CRC and CCA was low as compared to other reports from Asia and the West. The data presented in the current study provides a blueprint of the spectrum of PSC-IBD in India, which is disparate from that reported in the literature. More data is needed to describe the true spectrum and long-term outcome of PSC-IBD in India. To achieve this, it is important to recognize and carefully screen all IBD patients for PSC, as an early appropriate diagnosis is imperative to prevent complications.