INTRODUCTION
Thrombosis is a major complication in patients with inflammatory bowel disease (IBD), and those patients have an approximately 2- to 3-fold higher risk of developing venous thromboembolism (VTE) than the general population [1-3]. VTE has been associated with an increased risk of in-hospital mortality (odds ratio [OR], 2.50; 95% confidence interval [CI], 1.83-3.43) [4], and the mortality rate was estimated to be > 15% in the first 3 months if patients with IBD developed pulmonary thromboembolism [5]. Therefore, prevention of VTE is a relevant issue in patients with IBD. The risk of VTE is affected by disease activity and the treatment setting. Among patients with IBD, those with active disease are at a greater risk of developing VTE than those in remission (incidence rate ratio, 4.5; 95% CI, 2.6-7.8) [6], and hospitalized patients are also at higher risk of VTE than those in ambulatory settings [6]. According to the clinical guidelines for IBD in Western countries, prophylactic antithrombotic therapy is strongly recommended for all hospitalized patients with IBD [3,7,8]. In contrast to Western countries, the significance of routine prophylactic antithrombotic therapy in Asian countries remains controversial. A previous large-scale study investigating venous thrombosis among Asian patients with IBD revealed that Asian patients with IBD were at a relatively lower risk of VTE than those in Western countries [6,9,10]. Thus, the implementation of thromboprophylaxis in hospitalized patients has been weakly recommended to be based on risk factors in clinical guidelines published in Japan [11].
According to a nationwide Japanese study, the incidence of VTE among patients with IBD was 1.03% (102.5 per 100,000 IBD person-years) [12]. Although this incidence rate is lower than that in Western countries [6,13,14], it is not negligible. Thus, identifying patients at a high risk of developing VTE is important.
Many hospitalized patients with IBD require central venous catheter (CVC) placement for nutritional support and bowel rest during active disease or short bowel syndrome. This treatment is an essential option for patients with IBD. However, an indwelling CVC is considered a risk factor for thrombosis [15]. The incidence of catheter-related venous thrombosis in patients with IBD was 3.5 times higher than that in patients without IBD [16]. Several studies from Japan have reported that CVC placement is more common in patients with VTE than in those without VTE [17-19]. However, the extent to which CVC placement increases the risk of VTE among hospitalized patients with IBD without antithrombotic prophylaxis has not been fully assessed. Therefore, we aimed to investigate the risk of VTE development focusing on CVC placement in hospitalized patients with IBD under no pharmacological prophylactic antithrombotic therapy.
METHODS
1. Participants
This retrospective cohort study was conducted at Keio University Hospital in Tokyo, Japan. We searched the hospital database for all patients with ulcerative colitis (UC) and Crohn’s disease (CD). All patients admitted to the hospital for disease exacerbation from January 1, 2016, to December 31, 2020, were enrolled in the study. To evaluate VTE development after admission and in active disease situations, we excluded patients hospitalized for reasons other than IBD flares or discharged within 48 hours of admission, patients who already had thrombosis on admission, pregnant women, and those who were using anticoagulants within 30 days before admission.
2. Patient Characteristics and Laboratory Data
We collected patient characteristics and laboratory data from the medical records of hospitalized patients with IBD. The patient characteristics included age, sex, body mass index, disease duration, history of surgical bowel resection, disease extension categorized by Montreal classification, disease activity on admission (e.g., UC, partial Mayo score, CD, Harvey-Bradshaw Index), current smoking status, history of thrombosis, medical treatment during hospitalization (e.g., 5-aminosalicylic acid, prednisolone, immunomodulators, anti-tumor necrosis factor-α agents, vedolizumab, tofacitinib, ustekinumab, and calcineurin inhibitors), and laboratory data on admission, including white blood cell count, hemoglobin concentration, platelet count, and C-reactive protein (CRP), albumin, and D-dimer levels.
3. Central Venous Catheterization
To evaluate the association between CVC indwelling and the development of thrombosis, the patients were divided into catheterized and non-catheterized groups according to CVC insertion during the admission period. CVCs included both conventional CVCs and peripherally inserted CVCs.
4. Venous Thromboembolism
The patients were followed-up from the day of admission until discharge. The primary endpoint was VTE development during the hospitalization. Investigations for thromboembolism were performed in patients with suspected clinical symptoms according to the physician’s judgment during hospitalization. VTE was confirmed using ultrasonography or contrast-enhanced computed tomography imaging, regardless of the thrombus site. Contrast-enhanced computed tomography or ultrasonography was performed when patients were suspected of having VTE due to symptoms such as pain, redness, swelling of the upper or lower limbs, chest pain, respiratory distress, or obstruction of the CVC. This study also included cases in which VTE was detected incidentally on computed tomography or ultrasonography performed during hospitalization for diagnosis and evaluation of disease.
5. Non-Pharmacological Prevention for VTE
Non-pharmacological prevention for VTE such as mechanical thromboprophylaxis with compression stockings or intermittent pneumatic compression were provided for patients considered as high risk of deep venous thrombosis in lower extremity with the physician’s decision in each case referring to the clinical guidelines [20,21].
6. Statistical Analysis
Summary statistical tables were prepared using frequencies and proportions for categorical data and median and interquartile range for continuous variables to evaluate patient background. In a comparison of the baseline characteristics between the catheterized and non-catheterized groups, the Mann-Whitney test and Fisher exact test were used for continuous and categorical variables, respectively.
For the primary analysis, the incidence proportion and incidence rate of VTE were calculated. The incidence rate was expressed as 1,000 person-days. In cases involving multiple admissions, the cases were treated independently if the readmission was more than 7 days after the latest discharge. In cases of readmission within 7 days from the latest discharge, the 2 hospitalized periods were treated as the same admission period. When the patient was moved to another hospital, the observation was censored at the time of transfer. To reduce the selection bias between the catheterized and non-catheterized groups, the association between catheterization and VTE development was investigated with propensity score (PS) analyses. PSs were calculated using a multivariable logistic regression model, estimating the ORs for catheterization with the covariates as below; age, sex, disease (UC or CD), current smoking status, past history of VTE, past history of bowel resection, hemoglobin concentration, white blood cell count, platelet count, and serum CRP and albumin levels on admission. Goodness-of-fit of the PSs was evaluated using the Hosmer-Lemeshow test [22]. The catheterized and non-catheterized patients were matched in 1:1 ratio based on the PSs with the nearest neighbor matching method without replacement using the calipers of width equal to 0.2 of the standard deviation of the logit of the PS [23]. After matching based on PSs, the association between catheterization and VTE development during hospitalization was estimated using univariable logistic regression analysis.
We conducted 2 sensitivity analyses. First, multivariable logistic regression analysis in the pre-matching patients adjusted with PSs and catheterization as covariates. Second, we performed an inverse probability of treatment weighting analysis using PSs [24,25].
For the secondary analysis, we investigated the predictors of VTE development. Univariable logistic regression models were used to estimate ORs and 95% CIs to predict VTE development. All P values were based on the two-tailed hypothesis, and P<0.05 was considered significant. Statistical analyses were performed using the JMP version 16.0.0 software (SAS Institute, Cary, NC, USA), Stata version 17 (StataCorp, College Station, TX, USA), or SPSS software version 28.0 for Windows (IBM Corp., Armonk, NY, USA).
7. Ethical Considerations
This study complied with the Declaration of Helsinki (revised in 2013) and the Guidelines for Medical Research Involving Human Subjects (Japanese Ministry of Health, Labour, and Welfare). The study protocol was reviewed and approved by the Ethics Committee of Keio University (approval No. 20150210). All data were collected anonymously. Written informed consent was not required due to the retrospective study design.
RESULTS
1. Baseline Characteristics
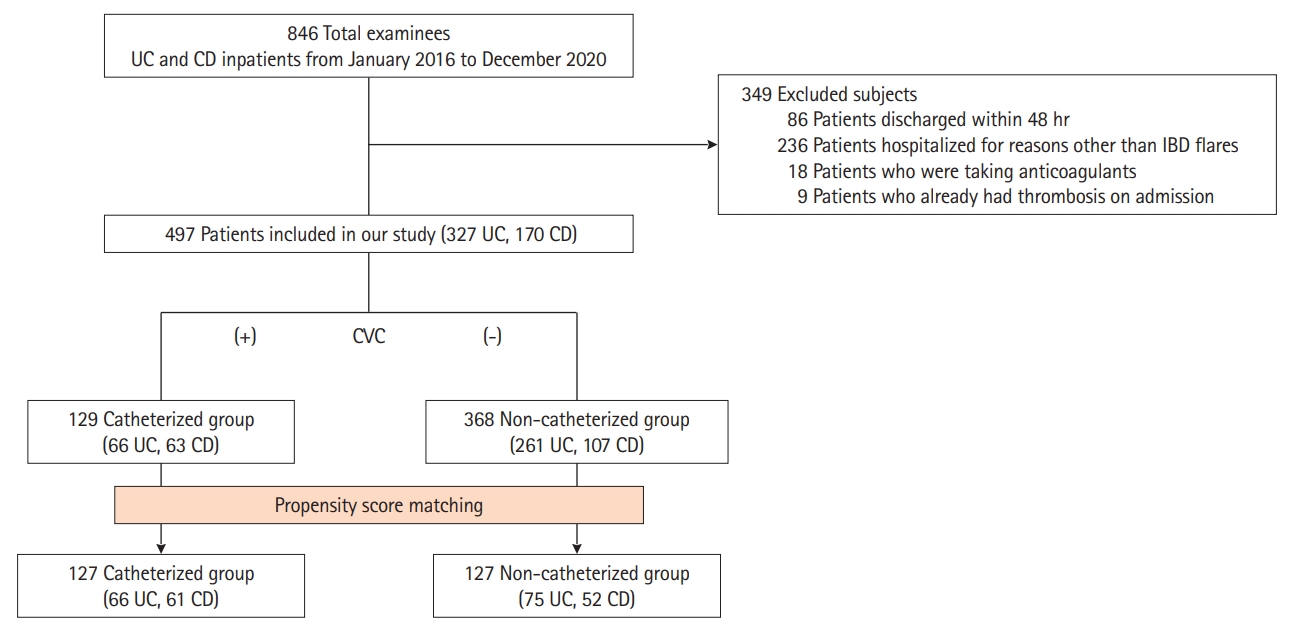
A total of 846 patients with IBD admitted to Keio University Hospital in Japan from January 1, 2016 to December 31, 2020 were eligible (Fig. 1). Two hundred thirty-six patients that were admitted for reasons other than disease flares, 86 patients that were discharged within 48 hours from admission, 18 patients who had received anticoagulants within 30 days prior to admission, and 9 patients who already had proven thrombosis on admission were excluded. Finally, 497 patients (327 with UC and 170 with CD) were enrolled in the study (Fig. 1). Pharmacological prophylactic anticoagulant therapy was not administered to the patients on admission. The median observational period was 16 days (interquartile range, 9-26 days).
The baseline characteristics of all the enrolled patients are described in Supplementary Table 1. On the basis of CVC indwelling during hospitalization, the 497 participants were divided into catheterized (n = 129) and non-catheterized (n = 368) groups. The catheterized group included 66 patients with UC and 63 patients with CD, while the non-catheterized group included 261 patients with UC and 107 patients with CD. The patient characteristics in each group are presented in Table 1. The indications for catheterization were summarized in Supplementary Table 2.
2. PS Matching
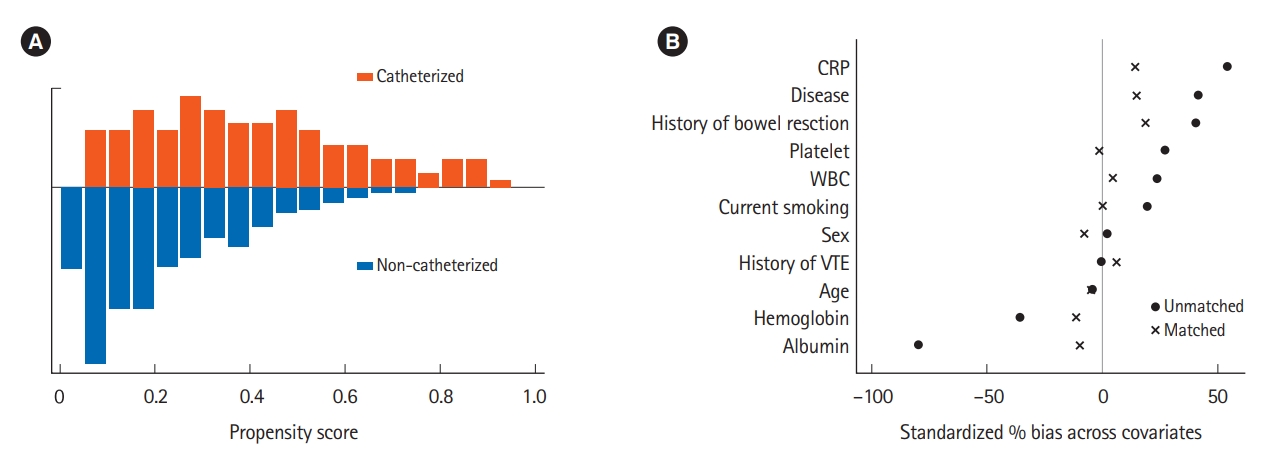
PSs were estimated in 482 patients with the exception of 15 patients in which the PSs were unable to be calculated due to missing data in covariates. The logistic regression model for the estimation of the PSs was valid (Hosmer-Lemeshow test, P=0.11), and the distribution of PSs is presented in Fig. 2A. The PS-based matching yielded 127 matched pairs (Fig. 1), and the variability of covariates used for estimating PSs was reduced after matching (Fig. 2B).
3. Association between Catheterization and VTE Development
The overall incidence of VTE development was 3.02% (15/497), and the overall incidence rate was 1.73 per 1,000 person-days during hospitalization. The mortality rate in this study was 0%. The cases that indicated VTE development included 9 cases (6 with UC and 3 with CD) of deep venous thrombosis in the lower extremities or pulmonary embolism and 11 cases (5 with UC and 6 with CD) of thrombosis related to CVC. VTE developed more frequently in the catheterized group than in the non-catheterized group (Table 2). The incidence of VTE was 9.30% (12/129) in the catheterized group and 0.82% (3/368) in the non-catheterized group. In the catheterized group, all the VTEs were developed after indwelling CVC. The incidence rate of VTE was 2.90 per 1,000 person-days in the catheterized group and 0.66 per 1,000 person-days in the non-catheterized group. After PS matching, an association between catheterization and VTE development was identified (OR, 13.15; 95% CI, 1.68-102.70; P=0.014).
4. Sensitivity Analyses
We conducted 2 sensitivity analyses. First, we adjusted PSs as the confounder and estimated the OR of catheterization for VTE development in the multivariable adjusted analysis among the pre-matching patients. Second, we used a univariable logistic regression model with inverse probability of treatment weighting. According to the 2 sensitivity analyses, the catheterization was also associated with VTE development (Table 3).
5. Exploratory Analysis for Prediction of VTE Development
We conducted an exploratory analysis to investigate the predictors of VTE development (Table 4). In the univariable logistic regression analysis, serum albumin level (OR, 0.28; 95% CI, 0.12-0.63; P=0.002) and hemoglobin level (OR, 0.79; 95% CI, 0.64-0.97; P=0.027) were associated with lower odds of VTE, while CRP level (OR, 1.08; 95% CI, 1.02-1.14; P=0.010) and platelet level (OR, 1.00; 95% CI, 1.00-1.01; P=0.025) were associated with higher odds of VTE. Treatment during hospitalization and disease (i.e., UC or CD) were not considered predictors of VTE development.
DISCUSSION
This study revealed that an indwelling CVC was a crucial risk factor for VTE development in patients with IBD hospitalized with disease flares. After PS matching, which reduced the effect of confounders such as disease severity between the catheterized and non-catheterized groups, the OR of catheterization to non-catheterization for VTE development was 13.15 (95% CI, 1.68-102.70), and similar results were also confirmed in 2 sensitivity analyses.
To the best of our knowledge, this is the first study to estimate the risk of VTE development focusing on CVC placement in hospitalized IBD patients with active disease using PS matching and inverse probability of treatment weighting analysis to adjust possible confounders, sufficiently. Previous studies investigated the risk of VTE in Asian patients with IBD, and found CVC placement to be one of the risk factors [9,17-19]. However, the degree of increased risk for VTE associated with indwelling CVC among hospitalized Asian patients with IBD has yet to be uncertain because of insufficient adjustment of potential confounders or lacking of data on the estimated risk to be increased for VTE in the past studies. The present study overcomes the limitations of the previous studies with the following strengths. First, we focused on the risk of VTE associated with CVC placement, and adjusted 11 possible confounders between catheterized and non-catheterized patients by using PS matching method and estimated the OR for development of VTE. Second, we conducted 2 sensitivity analyses with PS and the higher odds for VTE in catheterized patients were also confirmed. Third, the results of this study were independent to the effect of pharmacological thromboprophylaxis because patients under antithrombotic therapy were excluded from the study. In consideration of these points, the present study revealed that CVC placement was a crucial risk factor of developing VTE in hospitalized Japanese patients with IBD in active disease.
The incidence of VTE development in Asian countries is not more than that in Western countries; nevertheless, Asian patients with IBD are still at a high risk of VTE. In East Asia (Taiwan, Japan, and South Korea), the incidence of VTE in patients hospitalized with IBD was 0.9% [9]. According to a Japanese nationwide survey conducted by Ando et al. [12], the incidence of VTE in patients with IBD, including both inpatients and outpatients, was 1.03% (1.025 per 1,000 person-years [reported as 102.5 per 100,000 person-years]), and concluded that the risk of VTE in Asia was comparable to that in Western countries. In a large-scale longitudinal study conducted by Grainge et al. [6] in the United Kingdom (including 13,756 patients with IBD and 71,672 matched controls), the overall incidence of VTE was 2.6 per 1,000 person-years, which is higher than that in Japan [12]. The risk of VTE varies due to the difference in the settings where the patients are treated (e.g., ambulatory or hospitalization), and it might be affected by the patient composition in the study. Focusing on the admitted patients, Ananthakrishnan et al. [26] have reported that the incidence rates of VTE 30, 60, 90, and 180 days after the first hospitalization were 3.7/1,000, 4.1/1,000, 5.4/1,000, and 9.4/1,000 person-days, respectively. In the present study, the overall incidence proportion and incidence rate of VTE without routine pharmacological antithrombotic prophylaxis were 3.02% (15/497) and 1.73 per 1,000 person-days, respectively. The incidence of VTE among hospitalized patients with active disease in this study is lower than that in a study conducted in United States, although the incidence remains high.
The criteria for selection of Asian inpatients with IBD who should receive pharmacological antithrombotic prophylaxis are a relevant unsolved issue [9,27]. In the guidelines published in Western countries, prophylactic antithrombotic therapy is recommended to hospitalized patients with IBD because of their high risk of thrombosis development [1,3,7,8,28]. Meanwhile, the guidelines published by the Japanese Society of Gastroenterology state that the implementation of thromboprophylaxis in hospitalized patients with IBD should be determined by considering other risk factors and the increased risk of bleeding from the gastrointestinal tract and other organs associated with the intervention [11]. Venous catheterization, obesity, pregnancy, and recent surgery with general anesthesia have been considered minor risk factors for VTE in patients with IBD [1]. However, the present study revealed that the risk for VTE among Japanese hospitalized patients with IBD with active disease without thromboprophylaxis is much higher in those with CVC placement than in those without. Thus, hospitalized patients with active IBD in whom CVC is placed are at a high risk of VTE development, and thromboprophylaxis is to be considered proactively.
In an exploratory analysis, we determined that a low hemoglobin level, high CRP level, and low albumin level on admission were risk factors for VTE (Table 4). These results were consistent with those reported in previous studies [9,19,29]. All these factors are associated with high disease activity. Moreover, a low albumin level is considered a risk factor for thrombosis independent of inflammation [26]. The endothelial damage, which leads impaired function of the inhibition of platelet adhesion, the direct deposits of plasma proteins such as albumin, fibrinogen and von Willebrand factor, fibronectin on the surface of CVC itself, and hypercoagulability associated with the inflammation of underlying disease and sepsis or bacterial translocation into the blood stream have been reported as the possible mechanisms of thrombosis in conjunction with CVC placement [15].
This study had several limitations. First, this was a single-center retrospective study. The characteristics of hospitalized patients, such as disease severity, type of disease, and treatment, varied among institutions. Thus, selection bias should be considered during extrapolation. Second, we excluded patients in pregnancy, those with abnormal coagulation disorders and with prior thrombosis undergoing current antithrombotic therapy, and who were considered at a high risk of thrombosis. Therefore, evaluating the effect of these parameters on VTE development was not possible. Third, we could not access data on patients’ immobility which could be a potential confounder. Fourth, except for some cases in which it was incidentally detected, VTE was diagnosed mainly in patients who were suspected of having thrombosis based on the physician’s judgment. Thus, the incidence of VTE may have been underestimated because of the presence of asymptomatic thrombosis. Asymptomatic thrombosis is often observed in patients with IBD [19]. Future prospective multicenter studies are warranted to overcome these limitations and determine the incidence and possible risk factors for VTE associated with CVC in patients with IBD.
In conclusion, an indwelling CVC is a high-risk factor for VTE development in hospitalized Japanese patients with IBD with disease flares. In Asian countries, where thromboprophylaxis in hospitalized patients with IBD is to be considered together with the risk for thrombosis and adverse events due to antithrombotic therapy itself, preventive antithrombotic treatment would be beneficial for inpatients with active IBD in whom CVC is placed.